
Recent progress in lymphovenous anastomosis
 0
0 ,
, Abstract
Breast cancer-related lymphedema (BCRL) is a debilitating disorder affecting an estimated 1 in 5 women and men treated for breast cancer. Fortunately, super microsurgical techniques have advanced in recent years and now provide better options for the treatment of lymphedema, allowing timely surgical intervention that can delay or even prevent lymphatic degeneration. Lymphovenous anastomosis (LVA), a physiologic procedure that restores lymphatic drainage by connecting functioning lymphatic vessels with nearby veins, has been shown to be both minimally invasive and highly effective. The authors describe innovative approaches to LVA that will help optimize outcomes for patients with BCRL.
Keywords
INTRODUCTION
Breast cancer-related lymphedema(BCRL) is a frequent complication of axillary lymph node excision with adjuvant therapy, and affects both women and men diagnosed with breast cancer[1,2]. As secondary lymphedema is a progressive disorder that results in irreversible damage to the lymphatic vessels and surrounding tissue[3], patients should be encouraged to seek surgical advice in an early phase, particularly when refractory to initiated compression therapy[4]. While surgical treatment for lymphedema previously focused on ablative procedures, current surgical techniques for the treatment of lymphedema aim to restore the drainage of lymphatic fluid from the affected limb. Lymphovenous anastomosis (LVA) consists of an anastomosis between a lymphatic vessel and a subcutaneous vein, and because it allows the lymphatic fluid to drain into the systemic circulation, LVA has an immediate positive impact[5]. Furthermore, as LVA does not require harvesting of existing lymphatic tissue, the latter carrying an inherent risk of donor-site lymphedema, it is also a safe procedure[6]. Another advantage of LVA is that it requires only a small incision in the skin that can be performed under loco-regional anesthesia, resulting in a very low complication rate. Thanks to these advantages, LVA is particularly suitable as a first-line surgical option for the treatment of BCRL[7-9]. However, one must be aware that experience, together with specialized equipment, are prerequisites for a good patient outcome[10,11].
SURGICAL TECHNIQUE
The earliest series of LVAs in humans were described several decades ago[12,13], but the technique in current use was first developed by Koshima[14]. Supermicrosurgery refers to the handling of vessels with a diameter less than 1 mm, but the lymphatic vessels targeted in LVA are usually considerably smaller, between 0.20 and 0.80 mm in diameter. Several factors play a role in the outcome, including the incision location, the size and configuration of vessels, and the type of anastomosis.
An LVA skin incision is, on average, 2 cm in length and, despite directly interrupting superficial lymphatic vessels, does not provoke iatrogenic lymphedema. The location of the incision is based on the identification of lymphatics and veins during pre-operative assessment. Intra-operatively, the choice of suitable vessels can be challenging. Ideally, equally-sized vessels and/or vessels with favorable lymph-to-blood pressures should be used for the creation of the LVA. However, in case of a mismatch, several different approaches are available, ranging from venous-branch-plasty[15] and interposition[16] to funnelization[17] [Figure 1A]. The choice of a favorable recipient vein is also crucial[18]. It has been suggested that a relatively smaller subcutaneous vein should be selected for LVA when the lymphatic vessels are abnormally dilatated[5]. Particular importance should be paid to the prevention of blood reflux, for instance, by valvuloplasty[19], although[20] found no adverse effect on the outcome after blood reflux through anastomosis.
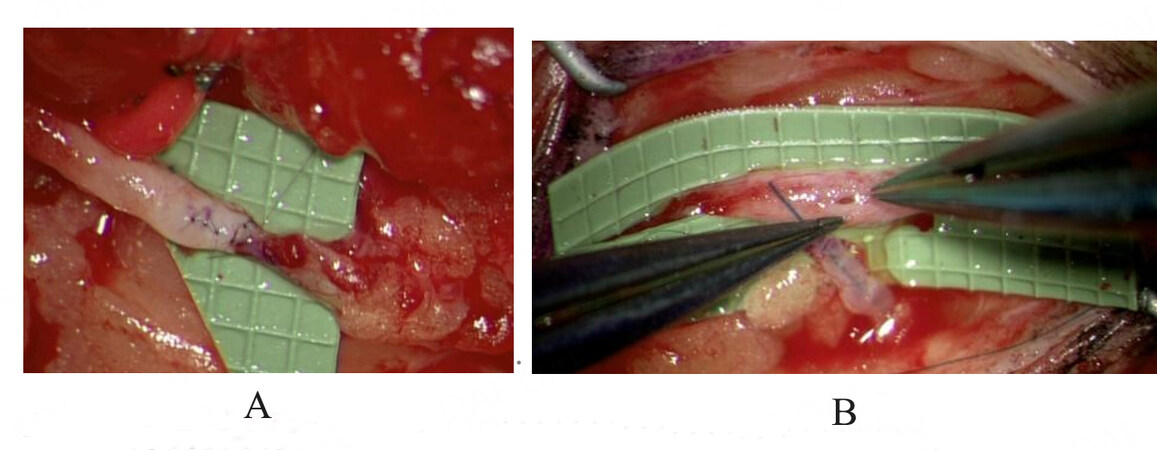
Figure 1. A: Funnelization of the vein; B: Intraluminal insertion of nylon stent in preparation for an end-to-side anastomosis.
The efficacy of LVA is also determined by the quality of available lymphatics. ‘Normal’ or ‘ectatic’ lymph vessels are preferred when creating a functioning LVA[11,21], although the true histopathology of the vessel is rarely known intra-operatively. An intima-to-intima approach is essential to prevent post-operative occlusions[5]. Intraluminal insertion of a custom-made nylon stent can help to avoid picking up the back wall, as well as to prove the patency of the LVA[22] [Figure 1B].
The patency of the LVA after anastomosis can now be easily confirmed through washout by lymphatic fluid in the vein and/or by observing indocyanine green (ICG) in the vein[23][Figure 2]. Indeed, thanks to the improvement in operative microscopes in terms of magnification and built-in infrared cameras, intra-operative visualization of lymphatic vessels is now common practice. Any leak can also be easily traced with the ICG module and should be rectified in order to prevent thrombosis. Before closing the incision, the position of the LVA and the vessels should be checked in order to optimize the long-term patency of the anastomosis: traction or aberrant position of the new construction should be avoided.

Figure 2. Peri-operative proof of patent anastomosis.
Depending on the available vessels preoperatively, a variety of anastomotic configurations can be created with the aim of increasing maximal lymphatic drainage into the venous system[23-25]. However, in the large majority of cases, an end-to-end anastomosis will be performed. Other configurations, including end-to-side, side-to-end, and side-to-side, are sometimes required, depending on the venous pressure and anatomy[26].
IMAGING AND EQUIPMENT
An already successful LVA procedure for lymphedema treatment can be further enhanced by the use of innovative technology and refined techniques[27]. While ICG lymphography is the gold standard for the identification of lymphatic vessels[28], deeper vessels (> 2 cm subcutaneously) cannot be visualized due to the limitations of current infrared cameras. The identification of lymphatics by ICG lymphography in patients with severe lymphedema is also limited due to the overlying dermal backflow. The implementation of super microsurgery for lymphedema treatment permitted the use of small vessels, an issue of particular importance in patients with BCRL who often present with swelling of the hand. Visualizing small lymph vessels in the distal region of the upper limb is paramount, as these vessels may allow anastomosis to low-pressure venules[14]. As LVA requires lymphatic vessels to be connected to nearby veins, the identification of suitable veins is obviously crucial.
The introduction of ultra-high-frequency ultrasound allows the detection of small-sized lymph vessels and veins in a non-invasive manner[29-31] [Figure 3]. While ultra-high frequency ultrasound has been revolutionary in the imaging of small-sized lymphatic vessels and veins, finding lymphatics with ultrasound in cases of severe lymphedema can nevertheless be challenging due to the limitations of coaptating contrast. Multispectral optoacoustic tomography (MSOT) is a 3D imaging modality based on the photoacoustic effect which allows exact spatial identification of (fluorescent) lymphatics and adjacent veins, thus overcoming these drawbacks[32] [Figure 4]. In a pilot study involving 11 patients, MSOT was found to accurately differentiate between distinct types of vessels including lymphatics, even in areas of dermal backflow, and provided images with high spatio-temporal resolution[33]. Of particular relevance to lymphatic surgery, we were able to successfully perform an LVA between an MSOT-identified lymphatic vessel and an adjacent vein[33]. In addition to identifying lymphatic vessels appropriate for LVA, photoacoustic imaging has also been used to confirm the post-operative patency of LVAs[34].
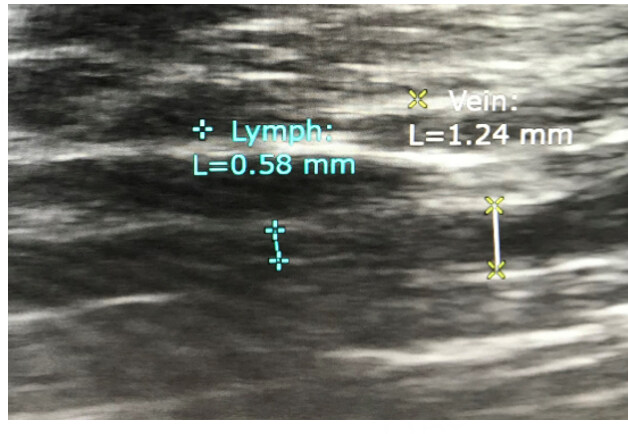
Figure 3. Visualization of lymphatic vessel and vein following ultra-high frequency ultrasound.

Figure 4. Visualization of lymphatic vessel (yellow) and vein (blue) in real-time following Multispectral optoacoustic tomography (MSOT).
The widespread application of super microsurgery, with its inherent focus on small-diameter vessels (0.1-0.3 mm), has also increased the demand for suitably-sized instruments [Figure 5] and needles[11] [Figure 6]. As all needles unavoidably cause tissue damage, with the extent directly related to needle size, fine needles are required for small and thin-walled lymphatics. For larger vessels, various 50 micron needles (suture size 11.0) are available and adequate. We recently reported on the use of a new 30 micron needle (suture size 12.0) in 20 LVAs in 10 patients with lymphedema of the limb[35]. Lymphatic vessels and veins had diameters of 0.2 to 0.4 mm and 0.3 to 0.8 mm, respectively. In total, 18 end-to-end and 2 end-to-side anastomoses were successfully performed.

Figure 5. Dedicated instrument: forceps.

Figure 6. Needles ranging from 50 microns.
Today, remarkable technological developments are underway, such as dedicated robots that have been successfully used for supermicrosurgical treatment of BCRL[36,37]. Furthermore, microscope-integrated laser tomography, which allows high-resolution assessment of the condition of the lymphatic lumen, is showing consideable promise[38].
UPPER EXTREMITY LYMPHEDEMA AND LYMPHORRHEA
Substantial evidence from a multitude of studies and reviews performed worldwide supports the efficacy of LVA for lymphedema of lower and upper extremities[39-42]. While immediate benefits include volume reduction of the affected limb, longer-term advantages include a decreased need for conservative therapy and compression garments, as well as a reduced frequency of infection[39,43,44].
LVA is typically used in the early stages of BCRL when a functional lymphatic system can still be identified. Early-stage lymphedema refers to excess volume caused by the accumulation of interstitial fluid. More advanced lymphedema is characterized by increased tissue fibrosis, hypertrophy of adipose tissue, and sclerosis of the lymphatic vessels, which are irreversible. While LVA is efficient in early-stage lymphedema, even late-stage lymphedema, typically treated by debulking procedures[45] or combined techniques[46], is increasingly being treated using LVA[47,48]. Alternatively, lymphatic vessel transplantation can reconstruct interrupted lymphatic pathways after axillary lymph node resection in patients with breast cancer[49].
In addition to arm lymphedema, breast lymphedema (BLE) is also a major sequela of breast cancer treatments[50]. Although an estimated one-third of all breast cancer patients develop BLE after breast-conserving surgery with axillary lymph node intervention, its management remains poorly described. LVA is reportedly effective for extremity lymphedema and also has proven efficacy in BLE[51,52]. While compression therapy is a cornerstone of the treatment of extremity lymphedema, in BLE, the complexity of breast shape causes significant difficulties. Given that patients with BLE mostly complain of (lymphatic) congestion, a newly created lymph-to-venous bypass will give immediate relief. As men may also develop BLE following breast cancer treatment, LVA can also be successfully performed in this group[53].
Axillary lymph node dissection in breast cancer treatment may also result in lymphorrhea. While lymphatic discharge generally ceases spontaneously, intractable leakage may result in a lymphocele or fistula and discomfort for the patient. Sclerotherapy or macroscopic ligation of the injured lymphatic vessels carries a risk of subsequent aggravating (clinical) lymphedema. Therefore, the anastomosis of a damaged lymph vessel to a nearby intact lymph vessel or vein is a physiological approach to restoring lymphatic drainage[54]. We have previously described the successful treatment of axillary lymphorrhea in a series of patients treated by LVA for intractable lymphorrhea[55].
DISCUSSION
Lymphedema surgery has evolved rapidly in the last decades, largely thanks to the introduction of super microsurgery and the application of ICG imaging. LVA is a physiological approach to lymphedema and is now well established as an effective and minimally-invasive surgical treatment for lymphedema without risk for complications[8,9]. LVA is safe and has an immediate post-operative therapeutic effect compared to other techniques including vascularized lymph node/vessel transfer. Consequently, LVA can now be considered the first-line surgical treatment for lymphedema, including BCRL. However, several remaining challenges need to be recognized.
Supermicrosurgery is technically difficult and a steep learning curve is inevitable. While major challenges such as vessel number and/or size mismatch or difficult vessel position may be encountered preoperatively, technological advances in equipment including microscopes and robotics allow LVAs to be performed with greater confidence.
How many anastomoses should be performed in order to obtain maximal lymphatic drainage is still a matter of debate[39,56]. And which factor is most important for success, the quantity or the quality (of vessels), also remains to be unequivocally established. On average, at least 3 LVAs are performed per patient, but factors including lymphedema stage and surgeon skill should also be taken into account[57]. Everyday practice, though, is determined by the number of vessels available for anastomoses and/or the reimbursement rules imposed by authorities or insurance companies. The exact location of a skin incision is also crucial for a good clinical result: the incision site is selected primarily on the basis of the ICG pattern, but for technical reasons, lymphatics and veins should preferably be in close proximity. Therefore, it is of the utmost importance that the surgeon has access to several (innovative) technologies/devices that facilitate the identification of vessels. This will be particularly beneficial in the case of patients with dermal backflow patterns and in patients with lymphedema of the hand, which is often an indication of degenerated lymphatic status. In addition to the indisputable role of near-infrared cameras, nowadays, ultrasound is also a prerequisite for good pre-operative assessment. More specifically, ultra-high frequency ultrasound can accurately detect (histologically confirmed) functional lymphatic vessels, even in advanced cases[58]. Lymphoscintigraphy is a reliable tool in the visualization of lymphatic function but well-known disadvantages, such as the two-dimensional view and the lack of projection onto anatomical landmarks, can be overcome with the use of lympho-SPECT/CT, which provides integrated information on lymphatic pathways[59]. However, as with magnetic resonance imaging, these technologies do not provide real-time information, which makes them less suitable for pre-operative planning.
Another concern is the long-term patency of an anastomosis. Efforts to prove patency should be made during the intervention. Furthermore, post-operative patency can be confirmed by means of ICG lymphography, lymphoscintigraphy, lympho SPECT/CT, or photoacoustic lymphangiography[59]. According to one report, over 70% of patients had at least one patent anastomosis 12 months after intervention[60]. Notwithstanding the data on functioning LVAs, there is still no consensus in the literature as to which tool should be used to assess the post-operative clinical effect of LVAs. It should be stressed that many variables need to be taken into account when assessing the overall outcome after LVA, among which are the number of patent anastomoses, lymphedema staging, patient characteristics, the surgeon’s experience, and accessible equipment.
LVA is now an established treatment option for lymphedema in various parts of the body, but is also being increasingly used to treat a broad range of lymphatic diseases varying from lymphorrhea, a complication of lymph node excision, to generalized lymphatic anomalies mostly encountered in pediatric patients[61]. However, the question of whether prophylactic LVA after lymphadenectomy actually avoids the morbidity associated with lymphedema needs to be proven in high-quality studies with a long follow-up period[62-64]. New technologies that focus on lymphangiogenesis also appear promising and may contribute to the treatment of lymphedema in the near future[65,66].
CONCLUSION
Thanks to major innovations and refinements in existing technologies and techniques, the outcome of LVA has improved considerably in recent years. LVA is now an effective and safe procedure and thus has the potential to become the first-line surgical treatment for lymphedema, greatly benefiting patients experiencing BCRL.
DECLARATIONS
Authors’ contributionsMade substantial contributions to the paper: Giacalone G, Belva F
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationAll patients gave consent for participation and publication.
Copyright© The Author(s) 2023.
REFERENCES
1. DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol 2013;14:500-15.
2. Byun HK, Chang JS, Im SH, et al. Risk of lymphedema following contemporary treatment for breast cancer: an analysis of 7617 consecutive patients from a multidisciplinary perspective. Ann Surg 2021;274:170-8.
3. Barone V, Borghini A, Tedone Clemente E, et al. New insights into the pathophysiology of primary and secondary lymphedema: histopathological studies on human lymphatic collecting vessels. Lymphat Res Biol 2020;18:502-9.
4. Bianchi A, Salgarello M, Hayashi A, Visconti G. Breast cancer related upper limb lymphedema: approach and surgical management. Minerva Surg 2021;76:575-9.
5. Seki Y, Kajikawa A. Fundamental and essential techniques for supermicrosurgical lymphaticovenular anastomosis: the art of Isao Koshima’s supermicrosurgery. Plast Aesthet Res 2021;8:44.
6. Demiri E, Dionyssiou D, Tsimponis A, et al. Donor-site lymphedema following lymph node transfer for breast cancer-related lymphedema: a systematic review of the literature. Lymphat Res Biol 2018;16:2-8.
7. Brahma B, Yamamoto T. Breast cancer treatment-related lymphedema (BCRL): an overview of the literature and updates in microsurgery reconstructions. Eur J Surg Oncol 2019;45:1138-45.
8. Rosian K, Stanak M. Efficacy and safety assessment of lymphovenous anastomosis in patients with primary and secondary lymphoedema: a systematic review of prospective evidence. Microsurgery 2019;39:763-72.
9. Chang DW, Dayan J, Greene AK, et al. Surgical treatment of lymphedema: a systematic review and meta-analysis of controlled trials. results of a consensus conference. Plast Reconstr Surg 2021;147:975-93.
10. Yamamoto T, Yamamoto N, Kageyama T, et al. Technical pearls in lymphatic supermicrosurgery. Glob Health Med 2020;2:29-32.
11. Chen WF, Tuncer FB, Zeng W. Advanced Technical pearls for successful supermicrosurgical lymphaticovenular anastomosis. Ann Plast Surg 2021;86:S165-72.
12. Nielubowicz J, Olszewski W. Surgical lymphaticovenous shunts in patients with secondary lymphoedema. Br J Surg 1968;55:440-2.
13. O’Brien BM. Microlymphaticovenous surgery for obstructive lymphoedema. Aust N Z J Surg 1977;47:284-91.
14. Koshima I, Inagawa K, Urushibara K, Moriguchi T. Supermicrosurgical lymphaticovenular anastomosis for the treatment of lymphedema in the upper extremities. J Reconstr Microsurg 2000;16:437-42.
15. Yamamoto T, Giacalone G, Hayashi A. Microsurgical venous-branch-plasty for approximating diameter and vessels' Position in lymphatic supermicrosurgery. J Plast Reconstr Aesthet Surg 2016;69:1152-3.
16. Yamamoto T, Giacalone G. Lymphatic vessel grafting for prevention of venous reflux into a sclerotic lymphatic vessel in supermicrosurgical lymphaticovenular anastomosis. J Plast Reconstr Aesthet Surg 2016;69:e67-8.
17. Azuelos A, Yamamoto T. Recipient vein funnelization for supermicrosurgical lymphaticovenular anastomosis. Microsurgery 2020;40:618-9.
18. Visconti G, Salgarello M, Hayashi A. The recipient venule in supermicrosurgical lymphaticovenular anastomosis: flow dynamic classification and correlation with surgical outcomes. J Reconstr Microsurg 2018;34:581-9.
19. Akita S, Mitsukawa N, Kuriyama M, et al. External valvuloplasty for subcutaneous small veins to prevent venous reflux in lymphaticovenular anastomosis for lower extremity lymphedema. Plast Reconstr Surg 2013;132:1008-14.
20. Hara H, Mihara M. Effect of venous reflux on the surgical result of lymphaticovenous anastomosis. J Plast Reconstr Aesthet Surg 2020;73:1174-205.
21. Koshima I, Kawada S, Moriguchi T, Kajiwara Y. Ultrastructural observations of lymphatic vessels in lymphedema in human extremities. Plast Reconstr Surg 1996;97:397-405.
22. Narushima M, Mihara M, Yamamoto Y, et al. The intravascular stenting method for treatment of extremity lymphedema with multiconfiguration lymphaticovenous anastomoses. Plast Reconstr Surg 2010;125:935-43.
23. Yamamoto T, Yamamoto N, Azuma S, et al. Near-infrared illumination system-integrated microscope for supermicrosurgical lymphaticovenular anastomosis. Microsurgery 2014;34:23-7.
24. Ayestaray B, Bekara F. π-shaped lymphaticovenular anastomosis: the venous flow sparing technique for the treatment of peripheral lymphedema. J Reconstr Microsurg 2014;30:551-60.
25. AlJindan FK, Lin CY, Cheng MH. Comparison of outcomes between side-to-end and end-to-end lymphovenous anastomoses for early-grade extremity lymphedema. Plast Reconstr Surg 2019;144:486-96.
26. Mukarramah DA, Kageyama T, Sakai H, et al. Comparison of outcomes between side-to-end and end-to-end lymphovenous anastomoses for early-grade extremity lymphedema. Plast Reconstr Surg 2020;145:1112e-3e.
27. Pons G, Tang JB. Major Changes in lymphatic microsurgery and microvascular surgery in past 20 years. Clin Plast Surg 2020;47:679-83.
28. Yamamoto T, Yamamoto N, Doi K, et al. Indocyanine green-enhanced lymphography for upper extremity lymphedema: a novel severity staging system using dermal backflow patterns. Plast Reconstr Surg 2011;128:941-7.
29. Hayashi A, Giacalone G, Yamamoto T, et al. Ultra high-frequency ultrasonographic imaging with 70 mhz scanner for visualization of the lymphatic vessels. Plast Reconstr Surg Glob Open 2019;7:e2086.
30. Hayashi A, Visconti G, Yamamoto T, et al. Intraoperative imaging of lymphatic vessel using ultra high-frequency ultrasound. J Plast Reconstr Aesthet Surg 2018;71:778-80.
31. Hayashi A, Visconti G, Giacalone G, Hayashi N, Yoshimatsu H. Recent advances in ultrasound technology: ultra-high frequency ultrasound for reconstructive supermicrosurgery. J Reconstr Microsurg 2022;38:193-9.
33. Giacalone G, Yamamoto T, Belva F, Hayashi A. Bedside 3D visualization of lymphatic vessels with a handheld multispectral optoacoustic tomography device. J Clin Med 2020;9:815.
34. Suzuki Y, Kajita H, Kono H, et al. The direct observation of lymphaticovenular anastomosis patency with photoacoustic lymphangiography. Plast Reconstr Surg Glob Open 2021;9:e3348.
35. Giacalone G, Yamamoto T, Belva F, Hayashi A. Letter to the Editor: Comment on Chen WF, et al. Advanced technical pearls for successful supermicrosurgical lymphaticovenular anastomosis ( Ann Plast Surg . 2021;86(3S suppl 2): S165-S172). Ann Plast Surg 2022;89:473-4.
36. Mulken TJM, Schols RM, Scharmga AMJ, et al; MicroSurgical Robot Research Group. First-in-human robotic supermicrosurgery using a dedicated microsurgical robot for treating breast cancer-related lymphedema: a randomized pilot trial. Nat Commun 2020;11:757.
37. Lindenblatt N, Grünherz L, Wang A, et al. Early experience using a new robotic microsurgical system for lymphatic surgery. Plast Reconstr Surg Glob Open 2022;10:e4013.
38. Hayashi A, Yoshimatsu H, Visconti G, et al. Intraoperative real-time visualization of the lymphatic vessels using microscope-integrated laser tomography. J Reconstr Microsurg 2021;37:427-35.
39. Scaglioni MF, Fontein DBY, Arvanitakis M, Giovanoli P. Systematic review of lymphovenous anastomosis (LVA) for the treatment of lymphedema. Microsurgery 2017;37:947-53.
40. Forte AJ, Sisti A, Huayllani MT, et al. Lymphaticovenular anastomosis for breast cancer-related upper extremity lymphedema: a literature review. Gland Surg 2020;9:539-44.
41. Gupta N, Verhey EM, Torres-Guzman RA, et al. Outcomes of lymphovenous anastomosis for upper extremity lymphedema: a systematic review. Plast Reconstr Surg Glob Open 2021;9:e3770.
42. Gasteratos K, Morsi-Yeroyannis A, Vlachopoulos NC, Spyropoulou GA, Del Corral G, Chaiyasate K. Microsurgical techniques in the treatment of breast cancer-related lymphedema: a systematic review of efficacy and patient outcomes. Breast Cancer 2021;28:1002-15.
43. Sharkey AR, King SW, Ramsden AJ, Furniss D. Do surgical interventions for limb lymphoedema reduce cellulitis attack frequency? Microsurgery 2017;37:348-53.
44. Salgarello M, Mangialardi ML, Pino V, Gentileschi S, Visconti G. A prospective evaluation of health-related quality of life following lymphaticovenular anastomosis for upper and lower extremities lymphedema. J Reconstr Microsurg 2018;34:701-7.
46. Masia J, Pons G, Nardulli ML. Combined surgical treatment in breast cancer-related lymphedema. J Reconstr Microsurg 2016;32:16-27.
47. Cha HG, Oh TM, Cho MJ, et al. Changing the paradigm: lymphovenous anastomosis in advanced stage lower extremity lymphedema. Plast Reconstr Surg 2021;147:199-207.
48. Visconti G, Hayashi A, Bianchi A, Tartaglione G, Bartoletti R, Salgarello M. Lymphaticovenular anastomosis for advanced-stage peripheral lymphedema: expanding indication and introducing the hand/foot sign. J Plast Reconstr Aesthet Surg 2022;75:2153-63.
49. Baumeister RG, Mayo W, Notohamiprodjo M, et al. Microsurgical lymphatic vessel transplantation. J Reconstr Microsurg 2016;32:34-41.
50. Rönkä RH, Pamilo MS, von Smitten KAJ, Leidenius MH. Breast lymphedema after breast conserving treatment. Acta Oncologica 2004;43:551-7.
51. Giacalone G, Yamamoto T. Supermicrosurgical lymphaticovenous anastomosis for a patient with breast lymphedema secondary to breast cancer treatment. Microsurgery 2017;37:680-3.
52. Scaglioni MF, Meroni M, Fritsche E. Lymphovenous anastomosis (LVA) for treatment of secondary breast lymphedema: A case report and literature review. Microsurgery 2021;41:165-9.
53. Giacalone G, Yamamoto T, Belva F, et al. Successful treatment of breast cancer-related breast lymphedema by lymphovenous anastomosis in a male patient. Microsurgery 2019;39:360-3.
54. Yang JC, Yen YH, Wu SC, Lin WC, Chiang MH et al. Supermicrosurgical lymphaticovenous anastomosis as an alternative treatment option for patients with lymphorrhea. Plast Reconstr Surg 2019;144:1214-24.
55. Giacalone G, Yamamoto T, Hayashi A, et al. Lymphatic supermicrosurgery for the treatment of recurrent lymphocele and severe lymphorrhea. Microsurgery 2019;39:326-31.
56. Onoda S, Satake T, Kinoshita M. Relationship between lymphaticovenular anastomosis outcomes and the number and types of anastomoses. J Surg Res 2022;269:103-9.
57. Hanson SE, Chang EI, Schaverien MV, et al. Controversies in Surgical management of lymphedema. Plast Reconstr Surg Glob Open 2020;8:e2671.
58. Bianchi A, Visconti G, Hayashi A, Santoro A, Longo V, Salgarello M. Ultra-high frequency ultrasound imaging of lymphatic channels correlates with their histological features: a step forward in lymphatic surgery. J Plast Reconstr Aesthet Surg 2020;73:1622-9.
59. Lasso JM. Lympho-SPECT/CT as a tool to evaluate postoperative outcomes after LVA for lymphedema repair. Plast Aesthet Res 2020;7:30.
60. Wolfs JAGN, de Joode LGEH, van der Hulst RRWJ, Qiu SS. Correlation between patency and clinical improvement after lymphaticovenous anastomosis (LVA) in breast cancer-related lymphedema: 12-month follow-up. Breast Cancer Res Treat 2020;179:131-8.
61. Mihara M, Hara H, Shibasaki J, et al. Indocyanine green lymphography and lymphaticovenous anastomosis for generalized lymphatic dysplasia with pleural effusion and ascites in neonates. Ann Vasc Surg 2015;29:1111-22.
62. Boccardo F, Casabona F, De Cian F, et al. Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up. Microsurgery 2014;34:421-4.
63. Jørgensen MG, Toyserkani NM, Sørensen JA. The effect of prophylactic lymphovenous anastomosis and shunts for preventing cancer-related lymphedema: a systematic review and meta-analysis. Microsurgery 2018;38:576-85.
64. Rodriguez JR, Fuse Y, Yamamoto T. Microsurgical Strategies for prophylaxis of cancer-related extremity lymphedema: a comprehensive review of the literature. J Reconstr Microsurg 2020;36:471-9.
65. Wolf S, von Atzigen J, Kaiser B, et al. Is lymphedema a systemic disease? a paired molecular and histological analysis of the affected and unaffected tissue in lymphedema patients. Biomolecules 2022;12:1667.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Giacalone G, Belva F. Recent progress in lymphovenous anastomosis. Plast Aesthet Res 2023;10:22. http://dx.doi.org/10.20517/2347-9264.2022.115
AMA Style
Giacalone G, Belva F. Recent progress in lymphovenous anastomosis. Plastic and Aesthetic Research. 2023; 10: 22. http://dx.doi.org/10.20517/2347-9264.2022.115
Chicago/Turabian Style
Giacalone, Guido, Florence Belva. 2023. "Recent progress in lymphovenous anastomosis" Plastic and Aesthetic Research. 10: 22. http://dx.doi.org/10.20517/2347-9264.2022.115
ACS Style
Giacalone, G.; Belva F. Recent progress in lymphovenous anastomosis. Plast. Aesthet. Res. 2023, 10, 22. http://dx.doi.org/10.20517/2347-9264.2022.115
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 6 clicks
Cite This Article 6 clicks

 Like This Article 1
likes
Like This Article 1
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.