
Eyelid defect reconstruction

Abstract
Eyelid reconstruction remains one of the more challenging areas of the face to reconstruct due to its dynamic complexity. They play an essential role in protecting the globe, forming a barrier against trauma, excessive light, and pumping tears towards the nasolacrimal duct system. A critical understanding of the anatomy and soft tissue reconstructive options is essential to properly reconstruct the eyelid and maintain the functional and cosmetic components.
Keywords
INTRODUCTION
The eyes are the central aesthetic focus of the face. It is usually the area on the face that we focus on when conversing with people, which is why irregularities or asymmetries are noted much more readily than if they were located elsewhere on the body. Because of this, eyelid reconstruction remains one of the more challenging areas on the face to reconstruct.
The eyelids also play an essential role in shielding the globe, protecting against trauma, excessive light, and pumping tears toward the nasolacrimal duct system. Therefore, it is important to have a comprehensive understanding of eyelid anatomy so as to restore it as close as possible to presurgical parameters, including the functional and cosmetic components, while minimizing surgical morbidity.
ANATOMY AND PHYSIOLOGY OF THE EYELIDS
An intimate comprehension of anatomy is the main component of any successful operation. Eyelids have complex anatomy, comprising an array of skin, muscles, blood vessels, and nerves. In addition, the mobile nature of the eyelids along with their importance of the air-tear interface can create challenges for the reconstructive surgeon.
The normal eye has an elliptical shape with the lateral canthus positioned approximately 2 mm higher than the medial canthus. Senescence can cause inferior dystopia of the lateral canthus, in contrast to the medial canthus, which tends to have a more stable position throughout adulthood. The palpebral fissure is defined as the aperture between the upper and lower eyelids. The horizontal palpebral fissure measures 28-30 mm, while vertically, it measures around 8-12 mm.
For the purposes of reconstruction, the eyelid was broken down into two distinct anatomical lamellae. The anterior lamella contains skin and the orbicularis oculi, while the posterior lamella is comprised of the tarsal plate and the conjunctiva. A gray line is visible along both eyelid margins, which marks the junction of the two lamellae. Posterior to the gray line is the mucocutaneous junction at the meibomian gland openings. The lower eyelid has similar structures, except the retractor is the capsulopalpebral fascia, which is an extension of the inferior rectus muscle [Figure 1].
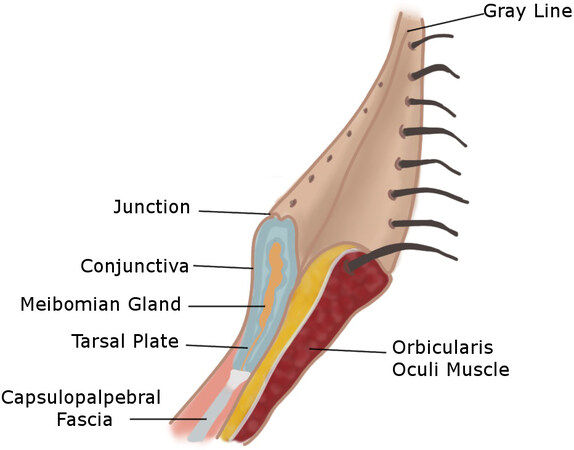
Figure 1. Anatomy of the lower eyelid.
The protractor of the eyelid is the orbicularis oculi muscle which is concentrically arranged around the palpebral fissure and divided into three segments. The pretarsal segment lies over the region of the tarsal plate and is responsible for involuntary blinking. Lastly, the orbital fibers are the outermost extension of the muscle and overlie the orbital rim, interdigitating with the frontalis muscle superiorly and the superficial aponeurotic system inferiorly.
The lateral canthal tendon functions as an anchor of the tarsal plates posteriorly and superolaterally to Whitnall’s tubercle. This ensures that the lateral eyelids abut the globe in all positions of gaze. The medial canthal tendon supports the lacrimal canaliculi and blends with the lacrimal sac fascia. The deep attachments of both canthal tendons need to be recreated in order to prevent malpositions of the eyelids.
Periorbital skin is the thinnest on the body and contains lower numbers of sebaceous glands than other areas. These glands produce sebum which lubricates and waterproofs the skin. Since there are fewer glands present, periorbital skin can tend to dry out and wrinkle faster. A lack of subcutaneous tissues beneath the thin eyelid skin means the skin tightly adheres to the underlying muscles, which are constantly contracting and transmitting movement to the delicate tissue.
Tear production and flow are essential components of orbital physiology. Tears are composed of three layers: an outer lipid layer, a middle aqueous layer, and an inner mucin layer. Tear drainage occurs via the lacrimal outflow system in each medial canthus. Epiphora, or excessive tearing, can be a problem after eyelid reconstruction due to an imbalance in the production and outflow systems. This can be caused by a reflex overproduction in response to a corneal irritation from a resulting eyelid malposition from the reconstruction. Damage to the lacrimal outflow system can cause an interruption in the tear drainage system.
Indications of eyelid reconstruction
Evaluation of eyelid defect
A preoperative analysis is essential to assess the possible areas for reconstruction to minimize surgical morbidity.
General consideration for lid reconstruction
Several factors determine the choice of reconstruction, including the nature of the defect, the availability of surrounding tissues, and the overall health and age of the patient.
The primary objective is to reestablish the function of the eyelids so that they are able to protect the eye with an equally important secondary objective of restoring the aesthetics of the eyelid. General treatment algorithms are detailed in Tables 1 and 2 below.
Treatment algorithm for full-thickness lower eyelid reconstruction
| Size of eyelid margin defect (% of eyelid width) | Type of repair |
| < 25% | Direct closure |
| 25%-50% | Direct closure with lateral cantholysis |
| 50%-75% | Tenzel semicircular advancement flap |
| > 75% | Hughes tarsoconjunctival flap |
Treatment algorithm for full-thickness upper eyelid reconstruction
| Size of eyelid margin defect (% of eyelid width) | Type of repair |
| < 25% | Direct closure |
| 25%-50% | Direct closure with lateral cantholysis |
| 50%-75% | Tenzel semicircular advancement flap |
| > 75% | Cutler-beard flap |
Some general principles are useful when approaching eyelid and periorbital reconstruction:
(1) If both the anterior and posterior lamellae need to be reconstructed, one must be composed of a flap that is well vascularized. Unfortunately, using a graft on graft reconstruction carries a high failure rate, likely due to a lack of vascular supply.
(2) If the inside of the eyelid is affected, it needs to be lined with nonkeratinizing mucosal epithelium to protect and lubricate the cornea.
(3) Allow for sufficient horizontal and vertical eyelid dimensions for maximal function in order to avoid vertical tension to the lower eyelid[1].
(4) Tissue match characteristics are critical for grafts and flaps.
(5) Ensuring adequate levator muscle function for the upper eyelid.
(6) Assessment of the lacrimal drainage system.
(7) To avoid corneal irritation, sutures should have knots on the cutaneous side.
Reconstruction of anterior lamellar defects
Primary closure
For anterior lamellar defects that solely require a simple ellipse for complete excision, primary closure can be performed, especially in the upper eyelid as this area frequently has redundant skin. The tissue adjacent to the defect should be released and undermined so that there is minimal tension on the wound closure. It is important to orient the closure parallel to the relaxed skin tension lines (RSTLs) while the ellipses in the periocular region should be oriented perpendicular to the RSTLs as this minimizes vertical tension and the risk of a cicatricial ectropion or lid retraction.
Laissez faire
The concept of healing by secondary intention is usually not a reasonable option for eyelid reconstruction, given the increased incidence of complications, including cicatricial ectropion. However, Fox and Beard[2] initially described this, and it has proven to be effective for relatively small medical canthal defects[3]. This region is concave and therefore tends to heal well if the defect is 1 cm or less in diameter and more centrally located between the upper and lower eyelids.
Local skin flaps
Skin flaps are the favored choice over skin grafts to repair anterior lamellar defects for several reasons[4]. Adjacent skin has a much better match for color and texture than grafts from distant sites like the commonly used retroauricular area. The robust blood supply allows the use of bare bone and can support free grafts for posterior lamellar reconstruction. Additionally, there is less contraction during healing which better supports the overall function of the periocular region.
Various flaps can be used in this region, orienting the vectors of maximal tension parallel to the lid margin. A rotation advancement cheek flap and lateral orbital flap are reasonable and useful strategies in addition to the options below.
Rhombic transposition flap
One of the most versatile flaps in the periocular area. The principle is shown in Figure 2A. The 60° to 120° rhombus can be thought of as two 60° equilateral triangles that are aligned at the bases. All sides are equal in length, and the designed flap is equal in size to the defect. After the transfer of the flap, the greatest wound closure tension is at the flap donor site[5]. This is important when considering possible distortion of the surrounding tissues.
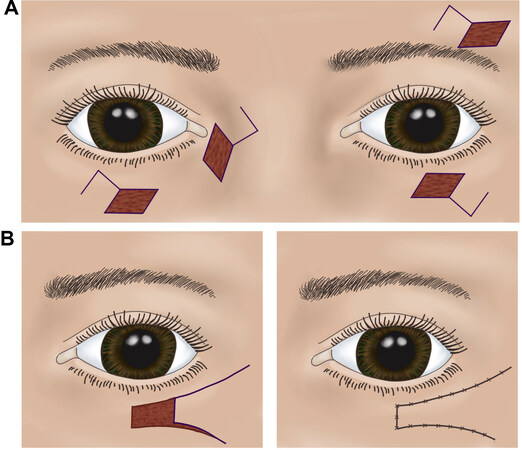
Figure 2. Local skin flaps. (A) Rhomboid flap. (B) Unipedicle advancement flap.
Unipedicle and bipedicle rectangular advancement flap
This versatile flap is appropriate for this area and used for defects as large as 25 cm2 [Figure 2B]. It can be particularly useful for defects in the medial upper and lower eyelids as well as those in the eyebrows. The resulting scar can be designed within the natural creases to avoid injury to the natural lid margin.
V-Y advancement flap
Tend to be useful for epicanthal folds and scar contractures. Their main function is to increase the length of the palpebral fissure.
Cervicofacial advancement cheek flap
The cervicofacial rotation advancement is a random-pattern flap that provides an excellent match for lid and cheek reconstruction. The incision runs from the superior aspect of the defect superolaterally to the preauricular cheek. The incision is then extended crossing under the ear and inferiorly along the lateral neck. The arterial supply arises from perforators of the facial and submental arteries. The cervical skin is an excellent source of redundant tissue and allows for proper tissue matching compared to a graft.
Reconstruction of full-thickness lid defects involving margin
Small defect (up to 25% to 50% of lid length)
The lids have an inherent ability to stretch, which is why it is usually possible to reconstruct small defects that involve 33% or less of the eyelid with direct approximation. This can be accomplished by conversion of the defect into a pentagonal defect with the vertical sides covering the height of the tarsal plate. This helps to eliminate dog ear deformities and also create a clean tarsal edge, avoiding misalignment or notching.
The most important suture is the approximation of the tarsus. 6-0 Vicryl suture is used to perfectly align the eyelid margin. An alternative to Vicryl can be monocryl or polydiaxonone. The lash line is then approximated with a 6-0 Vicryl followed by repair of the orbicularis oculi muscle. Both of these layers are crucial to minimize tension to the skin closure and maximize the appearance of the final scar. The skin is closed with a 6-0 nonabsorbable suture with nylon or polypropylene the preferred choices.
If there is some tension noted, particularly for the defects that range from 33% to 50%, a lateral canthotomy and cantholysis are performed to gain a few additional millimeters. Taking care to evert the lid margin wound edges will prevent a notched appearance to the eyelid when using the method of closure.
Tenzel semi-circular advancement flap
Medium defect (50% to 75% of lid length)
The Tenzel semi-circular advancement flap was originally described by Dr. Tenzel and Stewart[6] in 1978. It is a very useful technique to repair defects of the eyelid that are full-thickness, ranging from 33%-75% of the horizontal length of the lower eyelid and 30%-66% of the upper eyelid. The flap is a very similar concept to the Mustarde rotational flap but uses less tissue rearrangement to repair the eyelid lamellae. The benefit of this technique is that it is performed in a single-stage operation.
The Tenzel flap is most dynamic when lateral skin laxity is present based on its rotational design. Additionally, having small segments that are full-thickness on the eyelid can maximize the overall effectiveness of the flap. If no tarsus is present on the lateral side of the defect, incorporating a posterior lamellar graft such as auricular cartilage or hard palate mucosa[7], will help to achieve a more optimal result.
The flap is designed with an upward semicircular arching line that begins at the lateral canthus, measuring approximately 20 mm in diameter, when used for the lower eyelid [Figure 3A and B]. For the upper eyelid, a mirror image of the semicircular arch is used. Once the incision is made from the lateral canthus, a musculocutaneous flap is dissected followed by a lateral canthotomy with cantholysis of the inferior lateral canthal tendon [Figure 3C]. This adequately frees up the flap to allow for more rotation and mobilization into the defect. Meticulous approximation of the tarsal edges is essential to achieve a satisfactory cosmetic result. This is usually performed with 6-0 vicryl buried vertical mattress technique that can provide lid margin eversion. This can be followed by simple interrupted 6-0 Vicryl to further approximate the tarsus.
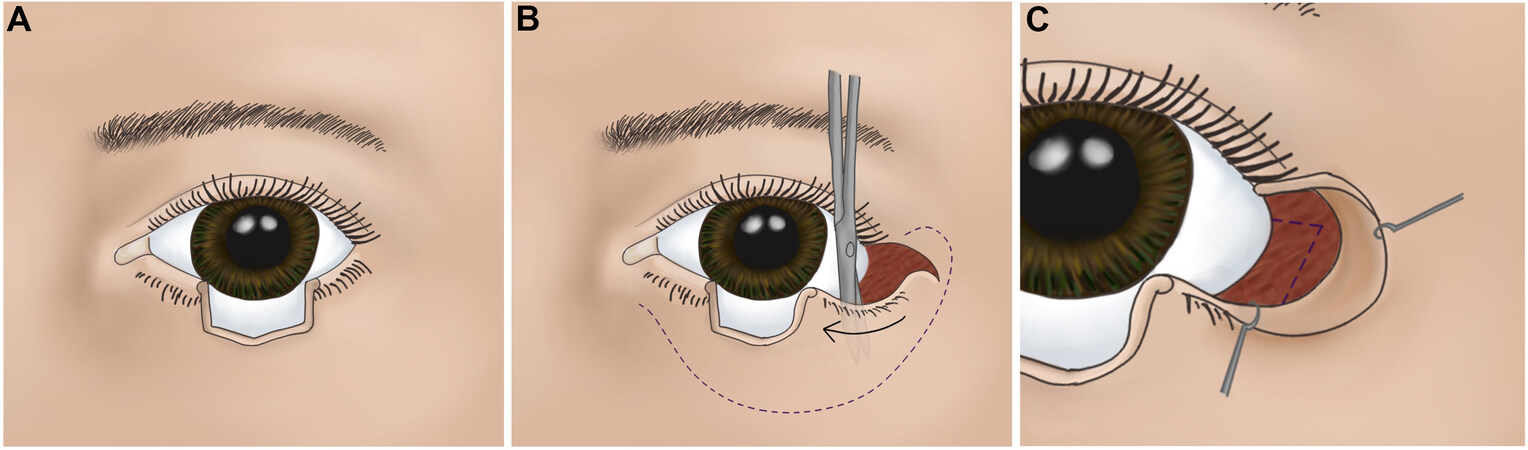
Figure 3. Tenzel flap. (A) Appropriate size defect for Tenzel flap; (B) flap that consists of skin and muscle is elevated and undermined as shown; and (C) lateral cathotomy and cantholysis are performed.
To address lateral sagging and malposition of the eyelid, the flap must be secured to the inner aspect of the superolateral orbital rim periosteum to form the lateral canthal angle. After the lateral support has been established, the remainder of the incision should be closed in layers, ensuring the muscle is approximated in a buried interrupted fashion. Skin is best closed with 6-0 polyproylene or nylon suture. Erythromycin ophthalmic ointment is the preferred wound care dressing.
Potential complications of the Tenzel flap can include ectropion, eyelid notching, lateral canthal webbing, trap-door deformity, and lack of eyelash in the lateral portion of the large defect.
Large defects (> 75% of lid length)
When addressing larger defects, the author understands that there is no clear percentage indication as an absolute for using one particular reconstructive option. This is dependent on factors that have previously been described, including the amount of eyelid laxity. Therefore, the percentages that are referenced are used as only a general guideline.
UPPER LID
Cutler-beard bridge flap
The upper eyelid anatomy is complex, given the dynamic nature of the upper eyelid. There are several factors involved in planning a reconstruction of a large defect to maintain function. These include corneal integrity, maintenance of vision and a range of movement of at least 5-10 mm for a dynamic blink. This is managed as a two-step reconstruction in which the tissues are first reconstructed with a secondary procedure to address the movement for vision and comfort to the eye.
The Cutler-Beard flap is a skin-muscle-conjunctiva flap that is advanced into the upper eyelid defect from the lower eyelid[8] [Figure 4A-C]. Because of the advancement of the composite flap to the upper eyelid, there is temporary closure of the affected eye for 4 to 6 weeks. The flap is designed with a full-thickness incision 1 to 2 mm below the inferior portion of the tarsal plate. This preserves the tarsus and also avoids the inferior marginal arcade, which maintains the vascularity of the flaps. The horizontal line is approximately 2 mm longer than the defect width, with the vertical lines extending inferiorly for 15-20 mm. The composite flap is then advanced under the intact inferior eyelid margin and sutured to the margins of the upper eyelid defect. The conjunctiva and lower eyelid retractors are first approximated followed by the orbicularis and skin. Some authors also describe the use of conchal/nasal cartilage grafts that are sutured to the remaining tarsus to provide rigidity[9]. After 4 to 6 weeks, the flap is separated as a second stage procedure. Following separation, the conjunctival edge is advanced and secured to the edge of the skin to ensure non-keratinization of the new upper eyelid and also to prevent any corneal erosions.
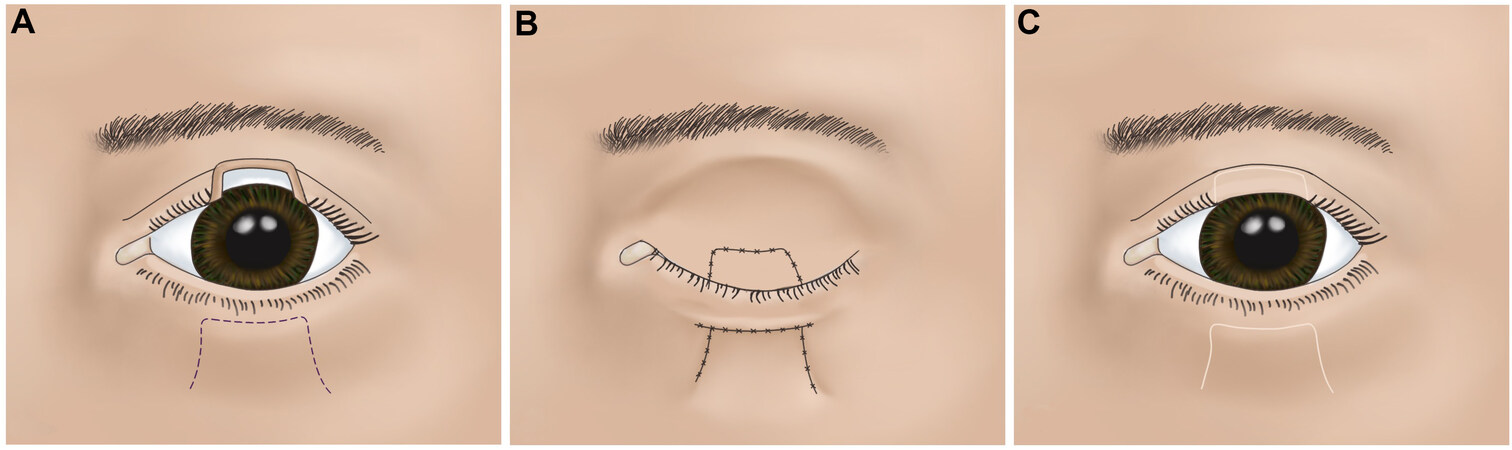
Figure 4. Cutler beard flap. (A) Flap design to the lower eyelid; (B) composite flap advanced under inferior intact eyelid margin; and (C) following separation of the flap.
Lower eyelid ectropion can occur as a result of denervation. Undermining the skin as well as the orbicularis can help to prevent this as well as performing a lateral tarsal strip procedure if needed.
LOWER LID
Hughes tarsoconjunctival flap
Hughes[10] first described this flap in 1937 to address larger, full-thickness defects involving 66%-100% of the lower eyelid. This is a two-stage flap that utilizes vascularized autogenous tarsus lined with conjunctiva from the upper eyelid to address the posterior lamella [Figure 5A-F]. The anterior lamella is reconstructed with either a full-thickness skin graft or a local advanced flap depending on how much laxity to the lower eyelid skin.
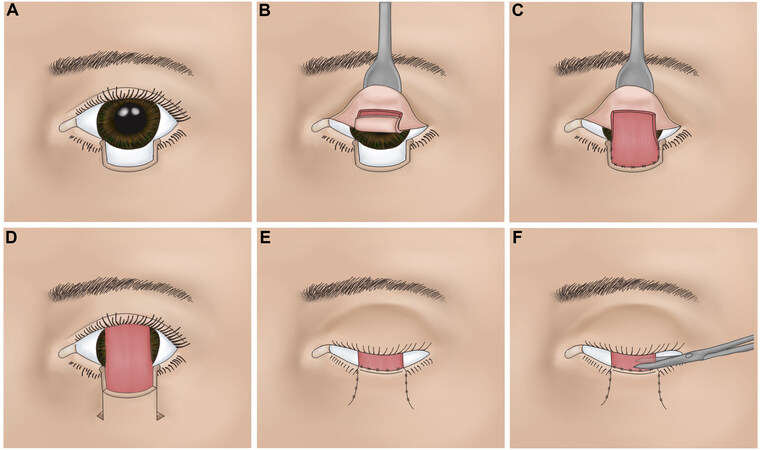
Figure 5. Hughes flap. (A) Appropriate size defect for a Hughes flap. (B) Conjunctiva and tarsus incised. Horizontal border of flap is at least 4 mm superior to lid margin. (C) Composite flap advanced into the lower lid defect. (D) Anterior lamella reconstructed with advancement flap. (E) Superior border or advancement flap suture 1 to 2 mm above upper border of tarsus. (F) Pedicle divided 4-6 weeks after initial reconstructive stage.
Local anesthetic is used to inject the recipient site as well the upper eyelid conjunctiva. Regardless of where the defect is present to the lower eyelid, the flap from the upper eyelid is raised centrally from where the tarsal plate has the largest vertical dimension. The width of the defect is measured, and when planning the tarsoconjunctival flap, it should be noted that it will be slightly narrower to allow for adequate horizontal tension in the reconstructed eyelid. The leading edge of the flap is 4 mm superior to the eyelid margin, which leaves a strip of tarsal plate for structural support.
The tarsoconjunctival flap is performed by everting the upper eyelid with a Desmarres retractor and carefully incising the measured markings. Dissection is performed with blunt-tipped scissors, as the levator aponeurosis is directly below this and should be left intact. Dissection is continued superiorly until there is enough length to advance the flap into the lower eyelid defect without any tension. The flap is secured with 6-0 Vicryl suture first to the medial and lateral edges followed by the inferior edge of the defect. Care should be taken to not include Mϋllers muscle within the tarsoconjunctival flap as the upper eyelid may retract after flap separation. Once this is secured and the flap is in position, the anterior lamella must be reconstructed.
The options for reconstructing the anterior lamella include a full-thickness skin graft or an advancement skin-muscle flap. The advantage of the latter is that there is an ideal color match to the surrounding tissues. However, the advancement flap is only possible when there is sufficient local tissue present which often is lacking with these types of defects. Skin graft donor sites commonly include the ipsilateral or contralateral upper eyelid and pre- or post-auricular skin. The full-thickness skin graft is harvested in the usual fashion and secured to the recipient site superiorly with 6-0 chromic gut. 6-0 silk can be used laterally and inferiorly to also incorporate into a tie-over bolster that is typically left in place for one week to ensure graft success.
The tarsoconjunctival flap is detached approximately at 2-4 weeks[11] after the initial reconstruction. Leaving a small cuff of excess flap is helpful so that the location of the mucocutaneous junction is anterior to the apex of the eyelid to provide protection to the cornea from any fine vellus hairs that are present on the skin graft. The conjunctival edge can be sutured with 7-0 chromic gut. Erythromycin ophthalmic antibiotic ointment is recommended twice daily for one week.
Potential short-term complications of the tarsoconjunctival flap include flap dehiscence, eyelid margin erythema and necrosis after division. Long-term complications include upper and lower eyelid retraction, notching of the reconstructed eyelid, ptosis to the upper eyelid, and entropion or ectropion. As an alternative to this flap, a recent case report has demonstrated modifications of the Tenzel flap to allow the closure of larger defects[12].
Canalicular repair
Canalicular injuries are commonly associated with lower eyelid avulsions. Defects that involve the upper and lower eyelids, including the medial canthus, will frequently involve the lacrimal drainage system. An attempt at primary reconstruction is always necessary to prevent epiphora and may involve more extensive procedures such as conjunctivodacryocystorhinostomy. Stents that are mono or bi-canalicular are the accepted approach to repair the canaliculi after the torn ends are identified.
CONCLUSION
Eyelid reconstruction remains one of the more challenging areas of the face to reconstruct due to its dynamic complexity. Thoroughly understanding the anatomy will aid the surgeon as to which reconstructive option is the best to maintain the functional and aesthetic components of the eyelid.
DECLARATIONS
AcknowledgmentsThank you to Olivia Abbatte for the talented and artistic illustrations provided for this chapter.
Authors’ contributionsThe author contributed solely to the article.
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestThe author declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationThe illustrations are originals by my illustrator. The copyright permission belongs to the author.
Copyright© The Author(s) 2022.
REFERENCES
3. Lowry JC, Bartley GB, Garrity JA. The role of second-intention healing in periocular reconstruction. Ophthalmic Plast Reconstr Surg 1997;13:174-88.
4. Patrinely JR, Marines HM, Anderson RL. Skin flaps in periorbital reconstruction. Surv Ophthalmol 1987;31:249-61.
5. Larrabee WF Jr, Trachy R, Sutton D, Cox K. Rhomboid flap dynamics. Arch Otolaryngol 1981;107:755-7.
6. Tenzel RR, Stewart WB. Eyelid reconstruction by the semicircle flap technique. Ophthalmology 1978;85:1164-9.
7. Jin MJ, Gao Y. Using buccal mucosa and auricular cartilage with a local flap for full-thickness defect of lower eyelid. J Craniofac Surg 2021;32:e660-1.
8. Shin HY, Chu M, Kim JH, Paik JS, Yang SW. Surgical feasibility of curtler-beard reconstruction for large upper eyelid defect. J Craniofac Surg 2019;30:2181-3.
9. Bartley GB, Kay PP. Posterior lamellar eyelid reconstruction with a hard palate mucosal graft. Am J Ophthalmol 1989;107:609-12.
10. Hughes WL. A new method for rebuilding a lower lid: report of a case. Arch Ophthalmol 1937;17:1008.
11. McNab AA. Early division of the conjunctival pedicle flap in modified Hughes repair of the lower eyelid. Ophthalmic Surg Lasers 1996;27:422.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Somenek M. Eyelid defect reconstruction. Plast Aesthet Res 2022;9:16. http://dx.doi.org/10.20517/2347-9264.2021.84
AMA Style
Somenek M. Eyelid defect reconstruction. Plastic and Aesthetic Research. 2022; 9: 16. http://dx.doi.org/10.20517/2347-9264.2021.84
Chicago/Turabian Style
Somenek, Michael. 2022. "Eyelid defect reconstruction" Plastic and Aesthetic Research. 9: 16. http://dx.doi.org/10.20517/2347-9264.2021.84
ACS Style
Somenek, M. Eyelid defect reconstruction. Plast. Aesthet. Res. 2022, 9, 16. http://dx.doi.org/10.20517/2347-9264.2021.84
About This Article
Special Issue
Copyright

Data & Comments
Data


 Cite This Article 7 clicks
Cite This Article 7 clicks

 Like This Article 1
likes
Like This Article 1
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.