
“R” face and neck lift: a modified technique for en-bloc facial rejuvenation

Abstract
Aim: We developed R lift, a modified en-bloc facelift, in response to growing demand for long-lasting, effective facelift procedures associated with minimal downtime and a low risk of complications. Conventional facelift procedures can be invasive, involve long recovery times, and can be disfiguring in the early postoperative period. However, nonsurgical modalities for facelift tend to yield a weaker, less noticeable lift and may require earlier revision.
Methods: Eighty-five patients who underwent R lift were evaluated retrospectively. Minor and major complications and the need for any revisions were recorded.
Results: Patients received follow-up for an average of 16.3 months (range 8-48.8 months). One patient required minor revisional surgery after dental abscess and subsequent soft-tissue infection of the face. Another patient had hypertrophic scarring. No patients experienced nerve damage or other major complications.
Conclusion: R lift is indicated for patients with the spectrum of age-related concerns of the mid/lowerface and neck. This technique yields reliable harmonious results, with a low risk of complications and a short recovery period. Continued follow-up data are needed to confirm the stability of the R lift result.
Keywords
Introduction
Conventional full facelift techniques encompass a range of dissections in competing tissue planes, ultimately with re-draping of tensioned fascial and/or skin flaps. There can be marked “down-time” to allow swelling, bruising, and scars to settle. More invasive facelifts, whilst proven to produce good to excellent results, also carry the potential morbidity of facial nerve injury and/or dysfunction[1]. Superficial musculoaponeurotic system (SMAS) facelifts in general target the scaffold of the facial (and neck) soft tissues and can include treatment of skeletal retaining ligaments. In recent decades, facelifts involving smaller incisions, suture-based techniques, and reduced undermining of the skin and underlying tissues have gained popularity[2].
Patients desire alternatives to traditional facelift that offer less downtime and a low risk of complications without compromising effectiveness or stability of the result[3]. This is exemplified in the boom of non-surgical facelifts and other treatments, which many patients prefer because the stigma of surgery is avoided. Herein, we describe a modified technique of composite facelift with minimal undermining-termed R lift-which we developed for patients who desire surgical rejuvenation of the face with a shorter recovery period. The incisions are greater than a traditional short scar procedure, but the footprint of surgical dissection is less than more invasive variants in our practice such as the deep plane lift. To avoid confusion with the multitude of acronyms and terminology we have simply used “R” in reference to the scar shape that mimics the lower case letter.
Methods
Patients and study design
This study was a retrospective appraisal of a consecutive series of R lift cases from inception. There were no exclusions to this series. Any patient having a primary or secondary R lift alone or in combination with other aesthetic procedures was included.
A total of 85 consecutive patients (79 women and 6 men) who underwent an R lift from April 2013 to December 2016 were evaluated in this retrospective study. Indications for this procedure were moderate jowl formation, marionette lines, and loss of the cervicomandibular angle (usually without platysmal bands). Prior to our development of R lift, patients with these features traditionally underwent minimal-access cranial suspension (MACS) facelift +/- open neck lift in our practice. The evolution of this technique was precipitated by a clinical situation where a standard MACS or SMASectomy facelift could have incurred significant skin necrosis in an Ehlers-Danlos syndrome patient detailed in previous work[4].
Eight patients were secondary cases (9.4%) whom had undergone previous facelift before inclusion in this study. Smoking was not an exclusion criterion, although patients were advised against smoking.
Surgical procedures
Skin laxity was assessed by digital palpation with the patient seated upright. Areas planned for excision are marked on the skin [Figure 1]. The mandibular angles are marked and the patient then placed supine (to mimic the surgical position) to ensure the neck markings for skin laxity create the correct cerviocmental angle when the skin is digitally manipulated in the face and neck lift vectors. Patients received either local or general anaesthesia, and prophylactic antibiotics (1.2 g amoxicillin/clavulinic acid or clindamycin 450 mg if penicillin allergy is present) were delivered intravenously at induction. Each side of the face was infiltrated with approximately 30 mL of diluted local anaesthetic [prepared by combining 90 mL of saline, 10 mL of 2% lidocaine, 0.5 mL of adrenaline (1:1000), and 2 mL of 8.4% sodium bicarbonate] in the subcutaneous plane. An incision was made along the pretrichial line in the temple and was extended caudally to the preauricular sulcus below the lobule and onto the posterior conchal skin two-thirds of the distance cranially and the skin excised onto SMAS [Figure 2].

Figure 1. Digital palpation and pre-operative markings in a 60-year-old woman with moderate ageing in the mid and lower face. The "x" marks the mandibular angle. The cervical line joining the mandibular angles is marked supine. Once supine the neck is digitally tightened to ensure the "x" marks correspond to the correct area for platysma plication. Otherwise if mal-placed anterior or posterior to this line, a neck deformity will ensue.
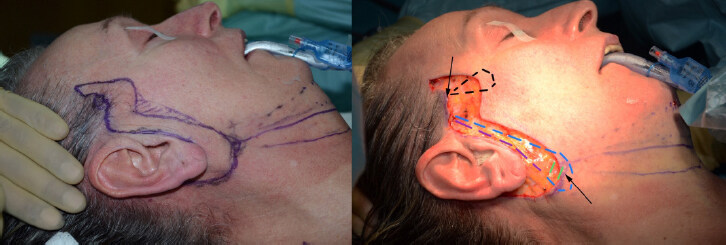
Figure 2. Excision of skin to expose the SMAS and platysma aponeurosis, in a 60-year-old woman. The 2 zones of minimal undermining are shown at the cranial pre-trichial region of the sideburn and the caudal extent of the platysma aponeurosis where the platysma is exposed (black arrows). The sequence begins with descent of the "U" suture (blue), before returning cranially two tangential platysmal bites (green) and then ascent to the temporal fascia (purple) for tying. Next the "O" suture is placed (black).
Skin regions marked preoperatively were excised to the SMAS anteriorly and the superficial temporal fascia cranially. The excision was continued subcutaneously in the retroauricular region and to the platysmal aponeurosis (i.e., the lateral extent of the platysma) in the infralobular region. Limited undermining was performed in 2 zones [Figure 2], approximately 2 cm in width from the margin of the cranial incision in the temporal region and in the infralobular zone caudally. To create an anchor point for the sutures, the deep temporal fascia was exposed just above the zygomatic arch at the prehelical incision site. Care was taken to preserve the temporal vessels. Similarly, the exposed platysmal region in the infra-lobular region is released from the sternomastoid fascia and the lateral edge of platysma freed along its exposed portion.
A series of sutures are performed, and the order is crucial to the result. First, a MACS “U” suture[1], was placed by means of 2-0 Ethibond suture material (Ethicon, Somerville, NJ). The U suture enables SMAS plication and runs caudally from the deep temporal fascia to the (now exposed) platysma at or anterior to the mandibular angle in the infralobular region, to return cranially [Figure 3]. Once the knot is tied the suture is kept long to complete the short dermal/SMAS suture after the “O” suture is completed. Just anterior to the temporal hair line at the level of the lateral canthus, a 1 cm area was undermined to expose the temporal fascia and a 2-0 Ethibond “O” suture was placed from here to the zygomatic SMAS and at the wound of the upper anterior cheek.
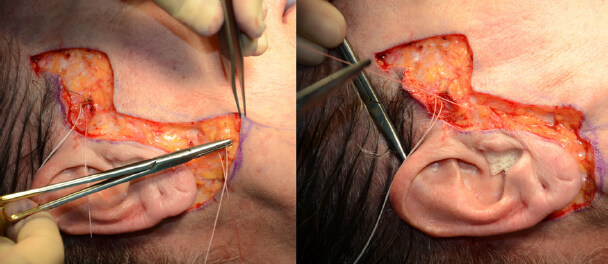
Figure 3. "U" suture into platysma at infralobular region in 60-year-old woman.
Next a series of up to three anchor sutures, but typically two, follow using polydioxanone sutures (Ethicon). These were placed from the platysma aponeurosis at the inferior margin of the incision to the platysma-auricular ligament in the infralobular region and from the SMAS and dermis at the incision margin-overlying the parotid gland-to the Lore’s ligament in the pretragal region. These sutures provide tension, directed obliquely to tighten the face and neck tissues as a composite of SMAS and skin [Figure 4]. Anchoring these sutures to fixed anatomic points that oppose the skin edges ensures tensionless closure of the dermis and skin. This creates a bunching effect in the pre-auricular region that is released by up to 1 cm undermining of the anterior skin flap. At this point the final Ethibond suture from the deep temporal fascia anterior to the helical root, a shortened “O” suture, is placed in the SMAS of the mid-cheek to complete the composite lift, contributing some oblique vector in addition to the vertical effect of the “U” suture [Figure 5].

Figure 4. Intraoperative photograph of this 60-year-old woman shows the subsequent suturing of the platysma aponeurosis/platysma to the platysma-auricular ligament (PAL), taking a bite of the former posterior to the already placed "U" suture (left picture showing base of ear closed). The next suture is marked by the blue marks that highlight the SMAS to Lore’s ligament anteriorly, after the PAL suture has been placed. PAL: Platysma-auricular ligament.

Figure 5. Intraoperative photograph of this 60 years old shows suture completion with the shortened ‘O’ suture.
Polydioxone sutures (Ethicon) then were placed posteriorly from the dermis to the fascia in the postauricular sulcus, another fixed anatomic site. This avoided stretching of the scar in the postauricular region. Placement of sutures in this order enabled approximation of the skin without creating an appearance of vertical neck folds for patients with significant skin laxity and accurate placement of the shortened “O” suture to allow accurate cheek lift.
Further dermal sutures using Monocryl (Ethicon, Somerville, NJ) were placed in the infralobular region to flatten the skin. Skin closure was achieved without drain placement. Adhesive strips (3M, Bracknell, UK) were applied along the suture line, and no other dressings were required. Patients were monitored for complications and need for revisional surgery in the early and late postoperative periods.
Results
The patients’ mean age was 59.9 years (range, 45-74 years). Fifty-five of the 85 patients (64.7%) were non-smokers. Forty-two (49%) underwent a concomitant aesthetic procedure at time of R lift [Table 1].
Adjunct procedures at time of R lift procedure
| Procedure | Frequency |
|---|---|
| Periorbital surgery | 29 (34.1%) |
| Neck liposuction/contouring/manipulation | 12 (14.1%) |
| Facial fat grafting | 1 (1.2%) |
| Breast surgery | 3 (3.5%) |
| Body contouring | 2 (2.4%) |
| Combinations of procedures | 5 (5.8%) |
Patients received follow-up for a mean of 2.5 years (range 0.7-4.5 years). One patient experienced dental abscess of a molar, which led to soft-tissue infection of the face 4 weeks postoperatively, and another patient experienced hypertrophic scarring that resolved after 1 steroid injection treatment (total 2.4% complication rate). This patient was treated by removal of the “U” suture while under local anaesthesia. None of the patients had any major complication, such as delayed healing, midface irregularities, facial nerve injury, or early relapse. In Figures 6-9, a patient is depicted preoperatively and in the early and late postoperative periods. These images highlight good correction of the lower face jowling, reduction in marionette prominence, improved contour of the central neck laxity, and minor banding. Furthermore, there is no scar migration and/or earlobe malposition.

Figure 6. A 71-year-old woman with moderate ageing pre-operatively.

Figure 7. The same 71-year-old woman in Figure 6, postoperatively at 1 week following R lift.

Figure 8. This 74-year-old presented with marked lower and mid face ageing and had a primary R lift. Pre-operative image on the left and 6-week postoperative appearance on the right.

Figure 9. The same 74-year-old with pre-operative and 6-week postoperatively left lateral view.
Discussion
We sought to develop a facelift technique that dramatically reduces morbidity without dramatic compromising of the result.
In the past, we recommended extended MACS lift for patients who did not require or wish to undergo facelift by means of full SMAS plication. Although MACS lift is associated with reduced postoperative morbidity, this procedure in our experience, and others[5], often results in nontrivial bruising. When we combined MACS lifts with open posterior cervicoplasty to address an unsatisfactory cervicomandibular contour, the early postoperative period occasionally involved significant swelling. In our practice, some patients who underwent MACS or extended MACS lifts experienced relapse of the neck deformity in as little as 2 years. In a clinical appraisal that matches our experience of MACs lift, Jacono and Parikh[6] specified that a key source of dissatisfaction with short scar techniques was unsatisfactory neck appearances. This manifested in their secondary facelift practice. Similarly, despite the advantages of MACS in other domains of patient goals (such as reduced downtime), subsequent modifications to MACS by its inventors resulted in modifications and adjuncts of the MACS (or extended MACS) procedure, in which the neck was more aggressively managed[7]. Tonnard et al.[2] felt there was a noticeable rate of poor neck contouring which required secondary surgery. We too have found this in our practice using either form of MACS procedure, hence the evolution of our modifications to better address the neck to create a more specific cervicomental improvement. Thus, to address variations in the aged face, our short scar procedure is a hybrid of techniques that are bespoke to the clinical issue for patients not willing to undergo a deep plane face and neck lift [Table 2].
Broad categories of adjunct procedures when treating patients with the R-lift technique in our practice
| Deformity | Procedure |
|---|---|
| Isolated jowl formation (e.g., slender runners) and mid facial/malar descent | R-lift only |
| Jowl, midfacial descent, and isolated central platysmal bands | R-lift plus medial cervicoplasty* |
| Jowls, midfacial descent, and blunted central neck (no cervicomental angle and no paramedian bands on animation) | R-lift, submental liposuction, and lateral platysmaplasty** |
Facelift procedures in the last 3 decades have involved various planes of dissection and treatment of distinct tissue layers of the face commensurate with the degree and type of aging in each layer. The skin and supra-SMAS layers respond to age-related facial changes with varied degrees of descent, volume loss, muscle atrophy, and attenuation/gravitational descent. The so-called finger-push facelift, commonly demonstrated in the clinic and described by Tonnard et al.[2], accurately represents a desirable facelift result because the skin and supra-SMAS layers can glide in an aged face. To our knowledge, investigators have not identified a region of maximum tissue mobility in the face that can be lifted for maximal effect. In addition, no studies have addressed concepts that produce ideal combinations of facelift techniques, for the competing facial tissues. Hence, like us, most aesthetic surgeons favour the tailored approach that works for them and the patients request, particularly their willingness to take on surgical risk and downtime.
As noted by Mendelson[8] the finger-push facelift manoeuvre does not result in a cheek deformity. This suggests that composite movement of the skin and SMAS may involve an equilibrium where liberation of SMAS, skin, and facial ligaments may not be wholly necessary. If the anterior masseteric ligaments are not divided, this deformity can still be avoided without applying less tension to the SMAS and overlying skin, provided the mild jowl deformity is corrected. Release is certainly required where a profound deformity of the lower and mid face requires correction. Certainly, in our practice sub-SMAS procedures are performed in the midface depending on the patient’s acceptance of risk profiles and what they specifically want from their rejuvenation journey.
The SMAS is distinct from the parotid/parotidomasseteric fascia[9,10,11] and is thicker laterally, especially in the region of disorganized fibrous adhesions over the parotid[12,13]. It is generally accepted that mobility is greatest in the midface, namely, anterior to the parotid. This is generally accepted in the surgical community. When tension is applied to the skin-SMAS composite medial to the parotid, contour of the lower face and neck does not dramatically alter. When we do not perform significant undermining of the skin, we can effect greater excursion of the en-bloc flap by pulling the SMAS over the anterior parotid region than by pulling the skin alone. This observation has been described by others[14] and suggests that mobility of the sub-SMAS layer allows lateral repositioning of the skin-SMAS composite even in areas of the cheek accessed, by avoiding extensive undermining. Jacono et al.[15] compared sub-SMAS and SMAS-plication facelifts and demonstrated that addition of lateral cervical release enabled greater lateral distraction of the neck tissues.
Lassus[16] determined that suture placement across the SMAS in combination with aggressive undermining of the skin produced facelift results that typically lasted 10 years before requiring revision. Ivy et al.[17] compared limited (lateral SMASectomy) or conventional SMAS lifts with extended SMAS lift or composite facelift for a series of patients who underwent different types of lift on either half of the face. These authors found no discernible differences among facelift procedures 1 year postoperatively. They concluded that more extensive facelift procedures were unwarranted for most patients[18], Facelift by means of less invasive techniques is associated with relatively low revision rates, which suggests patient satisfaction[8,18]. However, reporting and observational biases may be involved.
The dermis has stronger ligamentous insertions than the SMAS[19], and mobilizing the skin independently of SMAS disconnects this arrangement. To our knowledge, it has not been determined whether the biomechanical behaviour of the retaining ligaments changes after ligaments are repositioned in different tension vectors. It is possible that facial ligaments may become tighter (akin to ligamentous contracture in the limbs) or are further attenuated. It is unlikely we will ever find a way of accurately measuring this. Mendelson[8] noted that division of the mandibular retaining ligament is paramount for lifting an aged face. We suggest that if the ligaments are attenuated, they may be moved while retaining their connections to the soft tissue and skeleton, which may explain why we do not routinely observe abnormal contours of the midface in our cases (where retaining ligaments were not released). We and Alghoul et al.[20] have observed cases in which the mandibular cutaneous ligament retains a robust dermal insertion. Placing tension to correct the jowl without releasing the ligament can produce dimpling in such cases. Therefore, additional undermining would be necessary to manage the jowl. It is our experience that this represents a minority of cases.
Anatomic changes in the platysma are a primary cause of neck deformity. The platysma is bound to the cervicomental dermis by dense connective tissue[21]. The platysma-auricular ligament represents a continuum of aponeurosis of the platysma and SMAS overlying the angle of the mandible and at the lobule of the auricle[22]. Baker[23] demonstrated that this anatomic arrangement allowed for simultaneous lifting of the face and neck. Waterhouse et al.[24] and Fogli and Desouches[25] subsequently refined concomitant rejuvenation of the face and neck.
Jones and Lo[26] evaluated long-term results of primary facelift, including short-scar SMAS plication, SMASectomy, and platysmaplasty, and found that correction of the jowl and marionette lines was stable 5.5 years postoperatively, whereas signs of neck aging had reappeared. A higher incidence of neck relapse in plication versus excisional platysmaplasty also has been described[27].
R lift differs from other limited facelifts, such as S lift and Le soft lift[27,28] ,because we extend suture placement beyond the lobule to the superolateral neck. This creates additional rejuvenation where the SMAS is adherent to the thick lateral platysma. The SMAS and platysma are kept in continuity with the repositioned skin, and plication sutures are placed to effect composite lift of the mid face, lower face, and neck. Sutures anchor the SMAS to fixed fascia and ligaments. Additional sutures anchor the lateral platysma to the retroauricular fascia, platysma-auricular ligament, and the pretragal (Lore’s) fascia [Figure 5]. This provides stability to the neck and face without eversion or flattening of the auricle.
This modification is crucial for the restoration of a youthful cervicomandibular contour and removal of neck laxity, giving a smooth neck contour down to the supra-sternal region [Figures 6 and 7]. It is also useful, in this experience, for moderate to marked ageing of the lower face [Figures 8 and 9].
Ultimately long-term data for R lift are needed to ascertain whether signs of aging will re-emerge disproportionately. In the facial rejuvenation community, we are at the mercy of heterogenous procedures for heterogenous patterns of face and neck ageing. We have noticed an increasing demand for minimally invasive procedures that allow quick return to social activities. To our knowledge, no investigators have evaluated whether patients would prefer a facelift that offers minimal downtime but later requires revision or a facelift that involves prolonged surgical recovery but yields a more enduring result. In recent years our observation has been patients are increasingly seeking a lesser procedure that translates as less downtime. We have therefore adapted and scrutinised the short scar offerings to build hybrid procedures that we feel take the best “bits” from our repertoires. A patient willing to accept maximal downtime for maximal result is offered a deep plane face and neck lift in our practice. However, those patients are decreasing in number year on year. With the R lift and its adjuncts most patients can return to normal social activities at around 1 week postoperatively with the hair down to conceal the wounds. It is our general experience that for our extended MACS (historically) and deep plane cases, patients generally require up to 3 weeks or longer postoperatively, to allow swelling and bruising to settle to permit return to normal social activities.
For a patient with platysmal bands and other neck deformity [Table 2], we consider R lift alone to be insufficient to wholly treat the central neck. In certain cases whereby the central bands are easily obliterated by a finger face lift in the examination mirror, the key platysmal sutures are sufficient [Figures 6-9]. Less commonly adjuncts and additional neck manoeuvres are required [Table 2].
We suggest that R lift is safe, reliable, and easy to combine with other facial rejuvenation procedures. Thus far, these data demonstrate for our patients that this variant and evolution of the short scar spectrum of facelifts possibly provides a more lasting result. Early indications suggest stable results, measured by no patient desire for revision on follow-up, at a mean of 2.5 years thus far. Face Q assessment and independent photographic assessment will form part of future study to validate our results and this technique. We recognise our very low revision rate is subject to biases whereby patients may seek revisional surgery at a different practice.
Conclusion
We developed R lift in response to the growing number of patients who present to our clinics seeking surgical rejuvenation of the face and a short recovery period. This modified composite facelift involves minimal undermining and the anchoring of sutures to fixed anatomic sites. For patients with age-related facial concerns, R lift of face and neck can yield good results, low morbidity, and a short convalescence period. Although we offer the full cross-section of facial rejuvenation surgery, our patients are particularly attracted to the minimal morbidity and short down-time this procedure offers. Longer term follow-up is needed to validate the stability of our promising early results.
Declarations
Author’s contributionsWriting and editing this manuscript, and prospectively maintaining a database for retrospective data collection and assessment: Saleh DB, Brierley N, Riaz M
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflict of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateThis study was approved by the Newcastle Hospitals Ethics Committee.
Consent for publicationWritten consent and permission has been given for use of the photographic material in this manuscript.
Copyright© The Author(s) 2021.
REFERENCES
1. Rammos CK, Mohan AT, Maricevich MA, Maricevich RL, Adair MJ, Jacobson SR. Is the SMAS flap facelift safe? A comparison of complications between the Sub-SMAS approach versus the subcutaneous approach with or without SMAS plication in aesthetic rhytidectomy at an academic institution. Aesthetic Plast Surg 2015;39:870-6.
2. Tonnard P, Verpaele A, Monstrey S, et al. Minimal access cranial suspension lift: a modified S-lift. Plast Reconstr Surg 2002;109:2074-86.
3. Jacono AA, Malone MH, Lavin TJ. Nonsurgical facial rejuvenation procedures in patients under 50 prior to undergoing facelift: habits, costs, and results. Aesthet Surg J 2017;37:448-53.
4. Rollett R, Bramhall RJ, Khan MA, Riaz M. Facelift for an ehlers-danlos syndrome patient: a case report. Aesthet Surg J 2016;36:NP131-4.
5. Mast BA. Advantages and limitations of the MACS lift for facial rejuvenation. Ann Plast Surg 2014;72:S139-43.
6. Jacono AA, Parikh SS. The minimal access deep plane extended vertical facelift. Aesthet Surg J 2011;31:874-90.
7. Tonnard PL, Verpaele A, Gaia S. Optimising results from minimal access cranial suspension lifting (MACS-lift). Aesthetic Plast Surg 2005;29:213-20.
8. Mendelson BC, Wong CH. Surgical anatomy of the middle premasseter space and its application in sub-SMAS face lift surgery. Plast Reconstr Surg 2013;132:57-64.
9. Jost G, Levet Y. Parotid fascia and face lifting: a critical evaluation of the SMAS concept. Plast Reconstr Surg 1984;74:42-51.
10. Wassef M. Superficial fascial and muscular layers in the face and neck: a histological study. Aesthetic Plast Surg 1987;11:171-6.
11. Levet Y. Comparative anatomy of cutaneous muscles of the face. Aesthetic Plast Surg 1987;11:177-9.
12. Broughton M, Fyfe GM. The superficial musculoaponeurotic system of the face: a model explored. Anat Res Int 2013;2013:794682.
13. Stuzin JM, Baker TJ, Gordon HL. The relationship of the superficial and deep facial fascias: relevance to rhytidectomy and aging. Plast Reconstr Surg 1992;89:441-9.
15. Jacono AA, Parikh SS, Kennedy WA. Anatomical comparison of platysmal tightening using superficial musculoaponeurotic system plication vs deep-plane rhytidectomy techniques. Arch Facial Plast Surg 2011;13:395-7.
16. Lassus C. Cervicofacial rhytidectomy: the superficial plane. Aesthetic Plast Surg 1997;21:25-31.
17. Ivy EJ, Lorenc ZP, Aston SJ. Is there a difference? A prospective study comparing lateral and standard SMAS face lifts with extended SMAS and composite rhytidectomies. Plast Reconstr Surg 1996;98:1135-43.
18. Rossell-Perry P, Paredes-Leandro P. Anatomic study of the retaining ligaments of the face and applications for facial rejuvenation. Aesthetic Plast Surg 2013;37:504-12.
19. Moss CJ, Mendelson BC, Taylor GI. Surgical anatomy of the ligamentous attachments in the temple and periorbital regions. Plast Reconstr Surg 2000;105:1475-90.
20. Alghoul M, Codner MA. Retaining ligaments of the face: review of anatomy and clinical applications. Aesthet Surg J 2013;33:769-82.
21. Huettner F, Vasconez LO, de la Torre JI. Neck rejuvenation--anatomy and clinical correlation. Facial Plast Surg 2012;28:40-51.
22. O’Brien JX, Rozen WM, Whitaker IS, Ashton MW. Lore’s fascia and the platysma-auricular ligament are distinct structures. J Plast Reconstr Aesthet Surg 2012;65:e241-5.
23. Baker DC. Minimal incision rhytidectomy (short scar face lift) with lateral SMASectomy. Aesthet Surg J 2001;21:68-79.
24. Waterhouse N, Vesely M, Bulstrode NW. Modified lateral SMASectomy. Plast Reconstr Surg 2007;119:1021-6.
25. Fogli A, Desouches C. Less invasive face-lifting: platysma anchoring techniques. Clin Plast Surg 2008;35:519-29. vi
26. Jones BM, Lo SJ. How long does a face lift last? Objective and subjective measurements over a 5-year period. Plast Reconstr Surg 2012;130:1317-27.
27. Saylan Z. The S-lift: less is more. Aesthet Surg J 1999;19:406-9.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Saleh DB, Brierley N, Riaz M. “R” face and neck lift: a modified technique for en-bloc facial rejuvenation. Plast Aesthet Res 2021;8:10. http://dx.doi.org/10.20517/2347-9264.2020.207
AMA Style
Saleh DB, Brierley N, Riaz M. “R” face and neck lift: a modified technique for en-bloc facial rejuvenation. Plastic and Aesthetic Research. 2021; 8: 10. http://dx.doi.org/10.20517/2347-9264.2020.207
Chicago/Turabian Style
Saleh, Daniel B., Neil Brierley, Muhammad Riaz. 2021. "“R” face and neck lift: a modified technique for en-bloc facial rejuvenation" Plastic and Aesthetic Research. 8: 10. http://dx.doi.org/10.20517/2347-9264.2020.207
ACS Style
Saleh, DB.; Brierley N.; Riaz M. “R” face and neck lift: a modified technique for en-bloc facial rejuvenation. Plast. Aesthet. Res. 2021, 8, 10. http://dx.doi.org/10.20517/2347-9264.2020.207
About This Article
Copyright

Data & Comments
Data


 Cite This Article 10 clicks
Cite This Article 10 clicks

 Like This Article 14
likes
Like This Article 14
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.