
Optimization of tissue anchoring performance and mechanical properties of barbed sutures for flexor tendons repair
 0
0Abstract
Aim: The ideal flexor tendon repair should be reliable, simple and strong enough without impairing the tendon healing. Based on these requirements, we have imagined the use of a single barbed intra-tendinous suture for stumps connection. The aim of our research is to quantify the stress that the suture and barbs should withstand in order to ensure perfect stumps connections.
Methods: Seven different cross-section sutures were selected for the research study. One circular and 6 different elliptical shapes were defined according to the ratio of their minor and major axes (ρ = b/a). Barbs were designed with 3 different depths and 3 different cut angles. Thus, 9 different situations were considered for each suture geometry. Finally, 2 loading conditions were applied on each barb and tested in ANSYS Workbench using a finite element analysis technique.
Results: Studies showed that a barbed suture with 0.18-mm depth, 150˚ cut angle and ρ = 3 produced the lowest stresses within the barb itself, while a barbed suture with 0.18-mm depth, 160˚ cut angle and ρ = 4 demonstrated lowest stress within the entire suture.
Conclusion: The stress values in these two configurations are observed to be very close and both can fit a single barbed suture for tendon insertion and repair.
Keywords
Introduction
The flexor system of the fingers has a particular anatomy and a specific gliding process which contribute to the flexion and mobility of the different joints of the fingers. This flexor system is composed by two tendons, the flexor digitorum superficialis (FDS) and the flexor difgitorum profondus (FDP). They originate from their corresponding flexor muscles, cross the carpal tunnel at the wrist level and the hand palm. At the base of each finger, they enter the flexor sheath and end at the base of the second phalanx for the FDS and at the base of the third phalanx for the FDP. The flexor sheath is composed by five annular pulleys and three cruciform pulleys. The integrity of the whole flexor system “muscle, tendon, flexor sheath and pulleys” is crucial for a normal hand and fingers function.
The anatomical position of the FDS and FDP tendons is relatively superficial in the hand and fingers and any sharp skin laceration at this level may lead to the rupture of any of them or both[1]. Reconnection of the two stumps of the ruptured tendon is mandatory with respect to the initial shape if we aim to reproduce a normal function.
Techniques of flexor tendon repair are well established and they have been subject to a great number of research and comparison studies. Usually a core suture with two strands is performed using non absorbable material to hold the two stumps together followed by a circumferential running suture to redesign the external shape of the tendon[2]. The healing process of the tendon lasts one month and combines the intra-tendinous process known as “intrinsic” and the extra-tendinous one or “extrinsic” healing process[3]. If the intrinsic component is mandatory for the anatomical tendon restoration, the extrinsic one can generate adhesions with the surrounding tissues impairing the tendon gliding process. This phenomenon of adhesions is more marked and penalizing when the FDS and FDP are both injured and when the rupture is localized within the flexor sheath; the “no man’s land”[4].
To avoid this phenomenon of adhesion, a particular protocol of passive tendon mobilization can be applied in order to prevent the extrinsic healing to be constrictive[5]. But this tendon mobilization, even if it is passively produced and under protection, can lead to secondary rupture or creation of a gap in the zone of connection. For this reason, authors have proposed the use in the core suture multiple strands with 4, 6 up to 8 strands instead of only 2 in order to strengthen the tendon stumps connection and prevent from secondary rupture[6]. But more strands are used, more the vascularity of the stumps is reduced leading to the rupture and failure of the tendon repair.
In order to avoid the previously stated problems, we have imagined the use of a barbed suture device inserted into the two flexor tendon stumps. The barbs should have the ideal shape to anchor into the tendon structure and enough mechanical properties in order to maintain the stumps connected while performing the physical therapy courses.
This article is an original research study with different circular and elliptical cross sectional sutures provided with 9 different types of barbs “3 different depth of cut and 3 different angle of cut” aiming to define the ideal suture shape, the best elliptical cross sectional ratio and the most strong barb configuration for flexor tendon repair.
Methods
Geometry description
The suture used for this experimental study is modeled as a solid cylinder. A circular cross sectional suture was first selected a 0.4-mm diameter and a 10-mm length [Figure 1]. Different elliptical cross sectional sutures were considered according to two criteria: first, the total area of the ellipse is equal to that of the circle and second, the uncut area for both the ellipse and the circle is also the same.
Figure 1. Design of the suture sample used for the experimental study
The barb is created by performing an extruded cut in this cylinder using slot geometry. The dimensions of the slot were chosen in accordance to the finite analysis software in order to obtain feasible meshing and appropriate results.
As for the barb, a slither of the suture material was removed with a cut radius at the base of the barb of 0.005 mm. This was done in order to avoid high stress concentrations that arise due to the presence of sharp cuts in the geometry. Two variables were changed in this study: the depth of the barb and the cut angle [Table 1]. Thus, nine different cases were considered for each of the geometries proposed either circular or elliptical.
The two variables used for barbs design
| Variables | Value 1 | Value 2 | Value 3 |
|---|---|---|---|
| Depth of cut (mm) | 0.07 | 0.12 | 0.18 |
| Angle of cut (°) | 150 | 160 | 170 |
Defining elliptical cross sectional areas dimensions
Given that the cross-sectional area of the suture remains constant, the geometry of the ellipse was defined such that the total area of the ellipse is equal to that of the circular cross-sectional area.
Area of circle = π*r2
Area of ellipse =π*a*b
Area of ellipse = π*r2 =π*(0.4/2)2 = 0.12566 mm2
In addition to the circular cross-section suture selected (ratio = 1), we have considered 6 different ellipse geometries with the following ratios of minor to major axes (ρ = b/a): 0.25, 0.5, 0.75, 2, 3 and 4 such that the area of the obtained ellipse remains equal to that of the circle. In Table 2, we have listed the minor and major axes for all the suture geometries analyzed in this work.
Major "a" and minor "b" axes of the ellipses considered for the study
| a | b | ρ | 1/ρ |
|---|---|---|---|
| 0.4 | 0.1 | 4 | 0.25 |
| 0.34641 | 0.11547 | 3 | 1/3 |
| 0.2828 | 0.1414 | 2 | 0.5 |
| 0.2 | 0.2 | 1 | 1 |
| 0.1732 | 0.231 | 0.75 | 4/3 |
| 0.1414 | 0.2828 | 0.5 | 2 |
| 0.1 | 0.4 | 0.25 | 4 |
Defining depth of cut in elliptical cross sectional areas
Given that the uncut area of all suture geometries remains constant, thus the uncut cross-sectional area of the ellipse is equal to that of the circular part with the same depth of cut. Thus, the depth of cut for all elliptical geometries is calculated from the following equation of the area of an ellipse with a cut:
A = a*b*[π/2 + sin-1 (d/a)] + [b*d*(a2-d2 )0.5]/a
Where “d” is the length from the origin to the cut and “a” is the length of the major axis while b is the length of the minor axis [Figure 2].
Figure 2. Different parameters on the ellipse used for the calculation of the depth cut
For d = 0.07 mm, Acircle remaining = 0.11089 mm2 and the depths of cut are given in Table 3 as depth of cut 1. They are respectively depth of cut 2 for d = 0.12 mm, Acircle remaining = 0.093957 mm2 and depth of cut 3 for d = 0.18 mm, Acircle remaining = 0.0708185 mm2.
Different depth of cut for the different ratios "ρ" in the elliptical sutures
| ρ | Depth of cut 1 (d = 0.07) | Depth of cut 2 (d = 0.12) | Depth of cut 3 (d = 0.18) |
|---|---|---|---|
| 4 | 0.035 | 0.065 | 0.0901 |
| 3 | 0.04047 | 0.075 | 0.10397 |
| 2 | 0.04972 | 0.0917 | 0.12742 |
| 1 | 0.07 | 0.12 | 0.18 |
| 0.75 | 0.081 | 0.15 | 0.208 |
| 0.5 | 0.0993 | 0.1835 | 0.2548 |
| 0.25 | 0.1405 | 0.2595 | 0.3605 |
The uncut area is chosen in blue [Figure 3] and is equal in all 7 geometries for the same set of depths of cut. In addition the major and minor axes are chosen such that the areas of the ellipses are equal to that of the circle. The different geometry sets of the different elliptical sutures used for the experimentation are reported in Figure 4; they represent a total of 7*3*3 = 63 sets.
Figure 3. Different elliptical geometries with different ratios "ρ" selected
Figure 4. Summary of all geometry sets considered (7*3*3 = 63 sets)
Meshing
A static structural project is created in ANSYS and all the geometries drawn in SolidWorks are imported into DesignModeler. Meshing is performed under Mechanical in Workbench. Every geometry model used for the experimentation is meshed by using nodes and elements.
Stress convergence
In finite element analysis, it is known that for geometries with corners, convergence of the stresses can hardly be reached. Resolving to a finer mesh for the analysis might not be the proper solution to reach convergence. Thus, during meshing, a set of different mesh configurations was considered and the one chosen was found to ensure proper convergence of the stress in the model with an acceptable duration for the simulation [Figure 5].
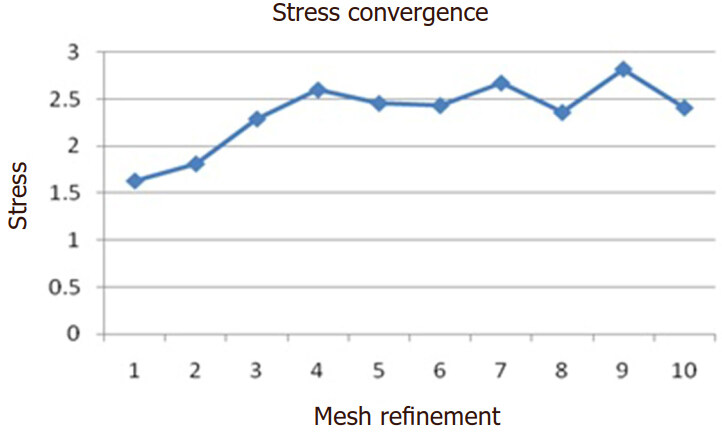
Figure 5. Converged stress versus mesh refinement
Different element sizing cases were considered without having either a fine relevance center or a refinement at the cut location. The values of the stress of the different cases of element sizing are depicted in Figure 5. The convergence curve is found to be acceptable since there are no diverging values of the stress; therefore, case 5 of the mesh refinement was considered since it ensured a fine mesh, with a converged solution and acceptable time for simulation [Table 4].
Mesh refinement analyzed in order to have the best stress convergence
| Mesh number | Refinement characteristics |
|---|---|
| 1 | Growth rate 1.4 |
| 2 | Growth rate 1.2 |
| 3 | Fine smoothing (growth rate 1.2) |
| 4 | Smooth transition (growth rate 1.2) |
| 5 | Virtual topology (growth rate 1.2) |
| 6 | Element sizing |
Meshing properties
Since the material considered is neoprene rubber which has elastic and plastic properties, a nonlinear analysis is performed with large deformations. Therefore, aggressive shape checking is specified in ANSYS Mechanical rather than standard shape checking. This ensures more conservative element shape checking criteria to account for possible distortion of the elements during the nonlinear analysis. In addition, the default volume mesher in ANSYS includes some defeaturing automatically. This will consequently lead to ignoring the small, narrow cuts. In our case, this is undesirable and thus the automatic mesh based defeaturing option was switched off.
On the other hand, a virtual topology is inserted. Including virtual cells properly merges our tiny edges into one edge for better meshing to preserve the rounded shape of the cut. Tetrahedral meshing in ANSYS is associated with virtual cells, allowing for a greater flexibility. Several meshing criteria are primarily considered in order to ensure proper stress convergence and a mesh independent problem. This is performed on one of the cases considered, 0.07 mm depth of cut and 150° angle of cut. In addition to the above defined meshing criteria, a growth rate of 1.2 is considered for better meshing results. This is defined with advanced size function on proximity and curvature. A sample of the actual meshing of the barbed suture is shown in Figure 6.
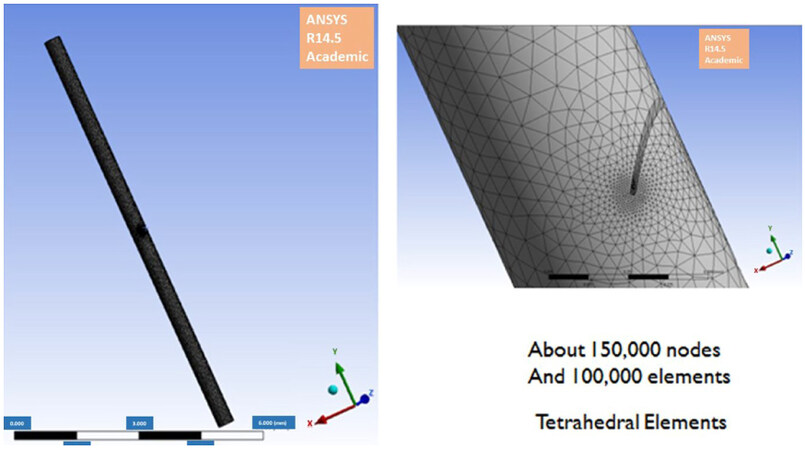
Figure 6. Sample of the final meshed geometry
Boundary conditions
Based on the actual scenario in vivo, two cases were considered. The first experimental situation consists of a fixed barb and a pulling force on the upper surface of the cylinder representing the suture with the second edge fixed [Figure 7], while in the second experimental situation, the same force is applied vertically downward on the barb itself with the two upper and lower surface edges of the cylinder are held fix [Figure 8].
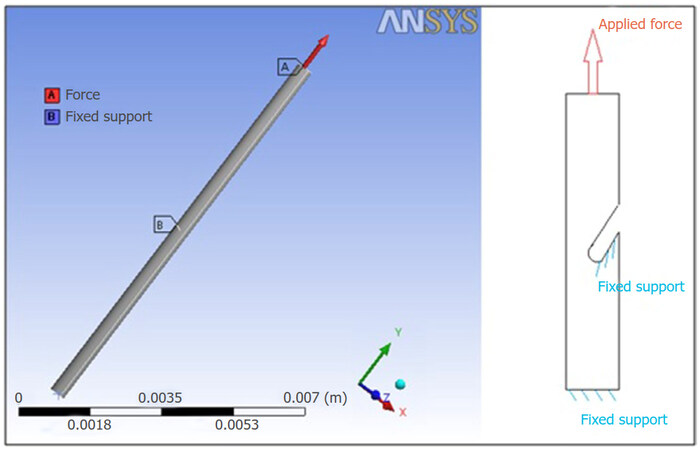
Figure 7. Pulling force is applied on the upper surface while the lower surface is fixed
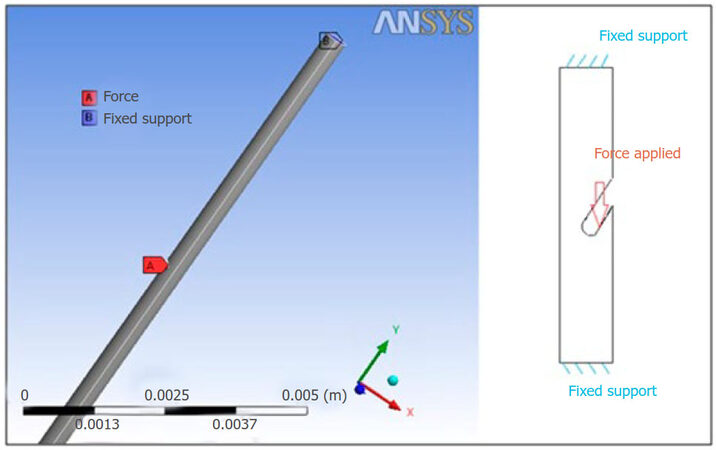
Figure 8. Upper and lower boundaries are fixed while the force is applied on the barb
Thus, the simulations for the above defined geometries were performed for each of the cases separately. Finally, concerning the material chosen to perform these different experimentations, neoprene rubber was selected since it showed similar elastic and plastic behavior to the actual material used for flexor tendons repair, the polypropylene.
In conclusion, seven different cross-section areas were considered with three different cut angles and three different depths of cut. Each of these cases was studied for the two boundary conditions of fixed barb and fixed edges. Thus, a total of 126 simulations were performed (7*3*3*2 = 126 simulations).
Results
After the proper mesh was assigned for the geometry, simulations for the circular cross-section area were analyzed. The equivalent Von Mises stress [Figure 9] and the maximal shear stress [Figure 10] obtained for the 18 different experimentations were recorded.
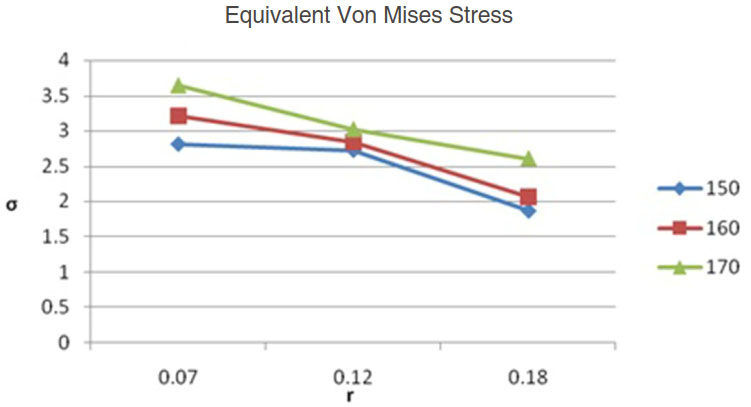
Figure 9. Circular cross sectional suture area Von Mises Stress
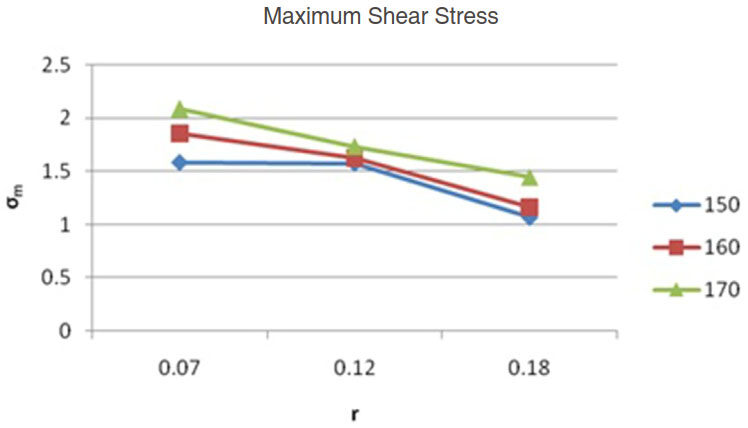
Figure 10. Circular cross sectional suture area Maximum Shear Stress
The suture with 150° cut angle and 0.18 mm depth of cut showed minimal Von Mises and maximum shear stresses when compared to the other configurations considered for a circular cross-section area.
Based on these preliminary results obtained from the circular suture different configurations, we moved to the analysis of the different elliptical sutures with the different preselected depths and cut angles barbs.
For the cut angle 170°, when the loading of the second situation was applied: depth of cut = 0.07 mm force was decreased by a factor of 10 [Figure 11]; and depth of cut = 0.12 mm force was decreased by a factor of 2 [Figure 12].
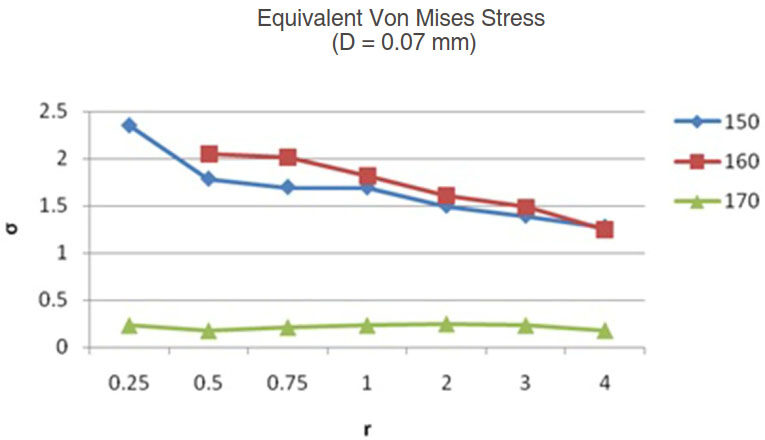
Figure 11. Equivalent Von Mises stress for d = 0.07 mm
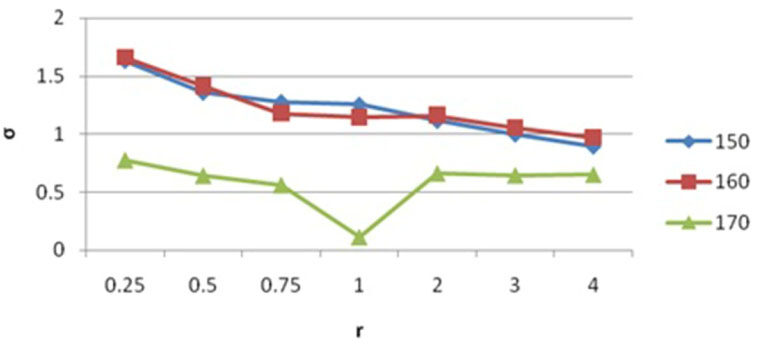
Figure 12. Equivalent Von Mises stress for d = 0.12 mm
It was noted that for the first situation, fixed barb with a vertical load applied on the upper edge of the cylinder, in all types of elliptical configurations, resulted in lower stresses. Furthermore, further investigation of the data showed that, the 0.18-mm depth of cut results in minimal Von Mises and maximum shear stresses. When compared with Ingle’s results for the circular cross sectional area, the ellipse with a ratio of major to minor axis equal to 3 (r = 3) is seen to have the lowest Von Mises and shear stresses as can be seen by the blue bars [Figure 13]. Nevertheless, when the complete set of data is analyzed, it is noted that with 160° cut angle, the ellipse with a ratio of 4 has even slightly lower values for the stresses [Figure 13]. When the second set of data is analyzed for the case of fixed surface and the load applied on the barb, the same results are observed also [Figure 14]. The blue bars showed the equivalent stress for 0.18 mm and 150° case, while the red bars show the equivalent stress for the 0.18 mm and 160° case.
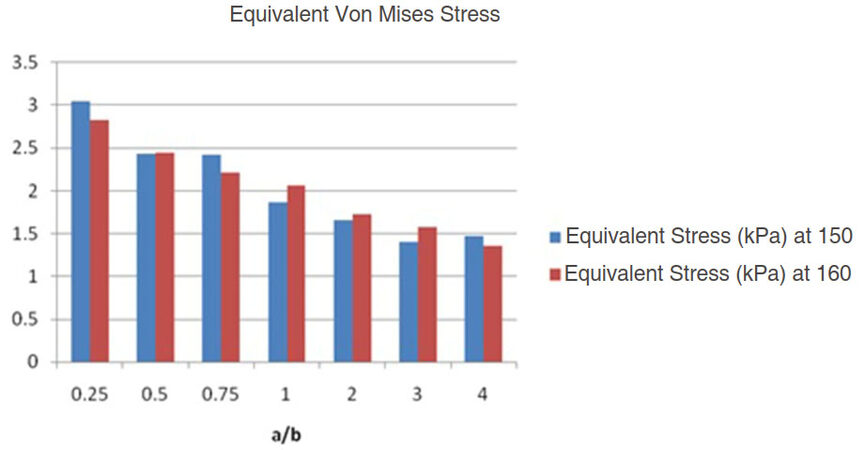
Figure 13. Equivalent Von Mises stress showing comparison between best ratios 3 and 4 for the first experimental situation of boundary conditions
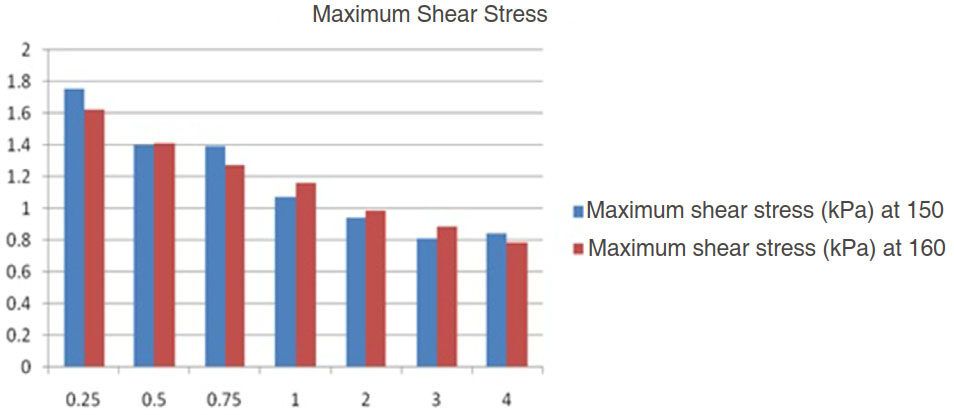
Figure 14. Equivalent Von Mises stress showing comparisons between best ratios 3 and 4 for the second experimental situation of boundary conditions
The results showed that as “r” of the elliptical cross sectional area increases for 0.18 mm and 150° case, the equivalent Von Mises stress will reach a minimum at r = 3 and then start to increase slightly after that at r = 4 [Figure 15]. However, for the case 0.18 mm and 160°, the Von Mises stress decrease to a minimum at r = 4 [Figure 16]. As r increases and since the area of the ellipse with a cut is calculated to be equal to that of the circle with the cut, and since the depth of cut were calculated for each case, the reason behind this improved behavior of the barb is due to the presence of more material in the barb, which is found at a certain maximal value, to sustain more load. On the other hand, the behavior of barbed sutures with elliptical cross sectional areas with r less than 1, a reverse behavior was observed. For r being 0.25, 0.5 and 0.75, higher Von Mises and maximal shear stress were obtained compared to the circular cross sectional area. Thus, they are not recommended for use in tendon repair.
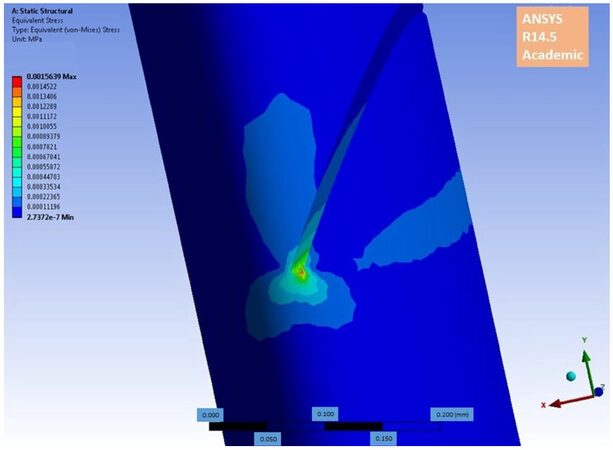
Figure 15. Equivalent Von Mises Stress r = 3, 0.18 mm, 150° Fixed Barb
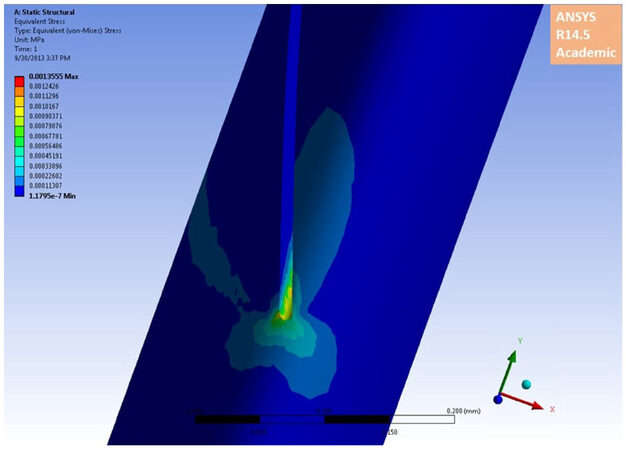
Figure 16. Equivalent Von Mises Stress r = 4, 0.18 mm, 160° Fixed Barb
Discussion
The work on barb sutures and anchoring devices dates back to 1945 with McKee[7] who described a device to join the detached ends of the tendon. The device consisted of a metal tube and small metal projections pointing towards the center of the tube. This technique was followed by another surgery to remove the tube. The target of the tube was to increase the strength of the repair by having the barbs hold the ends tight together and to decrease adhesion. However, high rates of adhesion formation and functional limitation were reported. Thus, a modified tool was proposed; nevertheless, there were no further accounts found on the use of this type of tool.
Another technique was launched by with Lengemann, an Austrian physician, in 1950 and was later introduced in the United States by Jennings and Yeager[8]. It was made up of a suture of braided tantalum wire with a V-shaped barb at one of its end to hold the tendon ends together and two soft buttons to maintain the suture ends on the surface of the skin. The suture and the barb at the end of healing are removed. Surgeons did not favor this technique due to the meticulous requirements for the barbwire insertion and the high risk of postoperative infection and skin irritation as the wire is still exposed for the whole period of tendon healing.
The first report for a nylon barbed suture was used by McKenzie[9] from New Zealand in 1967. This technique was introduced for the repair of finger flexor tendons. Two different configurations were suggested: form A consisted of unidirectional barbs with both ends of the suture kept on the surface of the skin and removed after four weeks while form B consisted of bidirectional barbs arranged in two opposing groups and intended to remain in the tendon after its repair [Figure 17]. In his report, McKenzie[9] reported that repair with 3-0 nylon barb suture can sustain a tensile strength of 17.8 to 26.7 N. This force is equivalent to that of the two strand Bunnell repair with stainless steel wire. Sutures were used for canine flexor tendons and healing occurred after 5 weeks of immobilization.
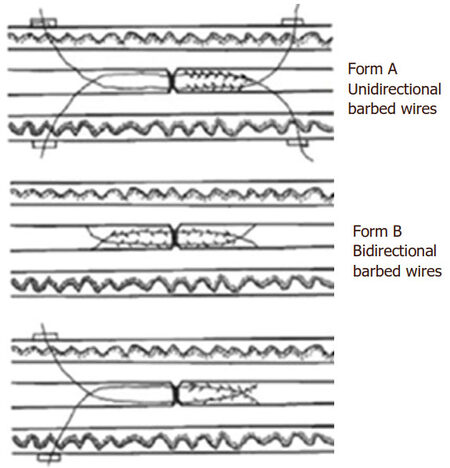
Figure 17. McKenzie barb sutures configurations (form A and B)
In London, one year later in 1968, Shaw[10] described the use of a barb wire suture, similar to that of McKenzie, consisting of a braided wire suture with sets of four straight metal opposing barbs pointing away from the needles at the ends [Figure 18]. In addition to the problem of immobilization during healing period, the experiments on dogs provided poor results. Thus, there was no further testing performed on patients.
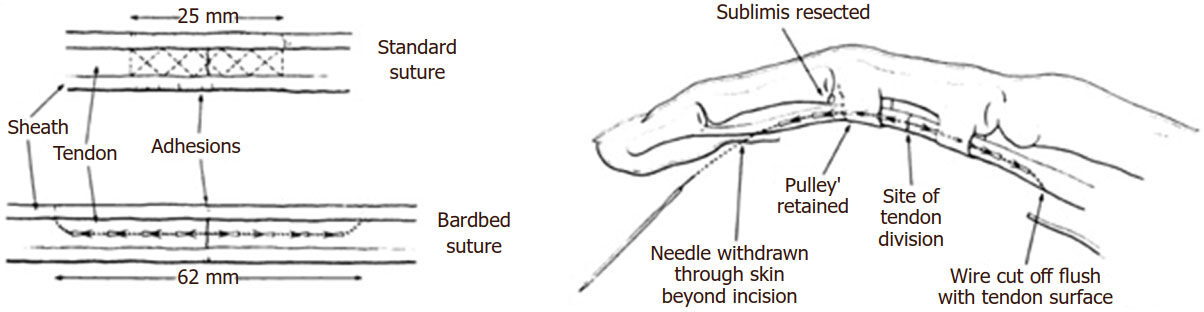
Figure 18. Shaw technique with the use of a bidirectional barb suture
More recently, in the International Conference and Exhibition on Healthcare and Medical Textiles in the United Kingdom in 2003, Leung[11] presented a bi-directional barb suture fabricated from a monofilament polydioxanone fiber, 17.78 cm long and 0.45 mm in diameter with 78 barbs in the middle present to escarp into the fiber [Figure 19].
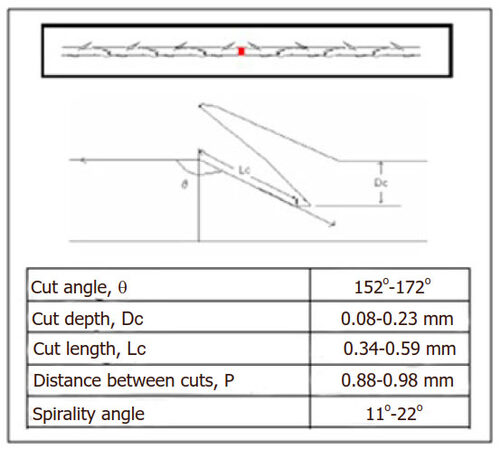
Figure 19. Magnified barbed suture with the geometry measurements of a single barb
The revival of barbed sutures and anchoring devices was launched by Su et al.[12], when they field for a patent on January 15th, 2008 for a device named Teno FixTM. This device has been used for zone II flexor tendon repair. It is composed of two intra-tendinous stainless steel anchors joined by a single monofilament 2-0 stainless steel suture. As it began to be used by surgeons, it was shown to withstand greater forces and to result in lower rupture rates than the traditional modified Kessler repairs [Figure 20].
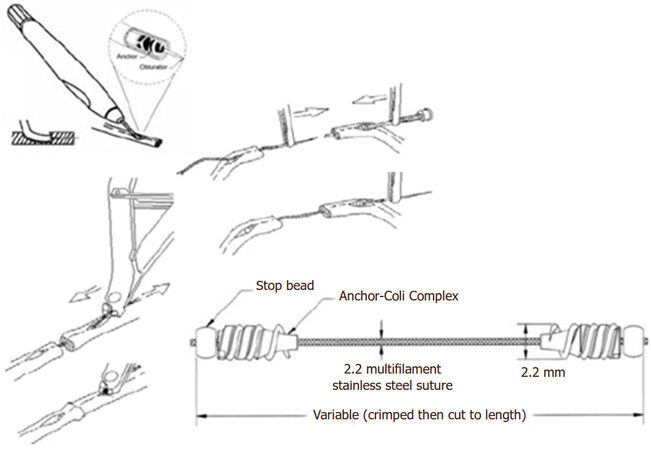
Figure 20. The Teno-Fix system
Another anchoring device was developed in 2010 by Hirpara et al.[13] formed of a pattern of anchors around the length of a nickel and titanium tube. The repair technique consisted of introducing the tube into one end of the divided tendon using a needle [Figure 21]. After half of the barbed tube reaches one end, the suture is pulled and the same procedure is repeated for the other end. When tested this device demonstrated ease of use and simplicity of the technique; however, it was not very clinically used.
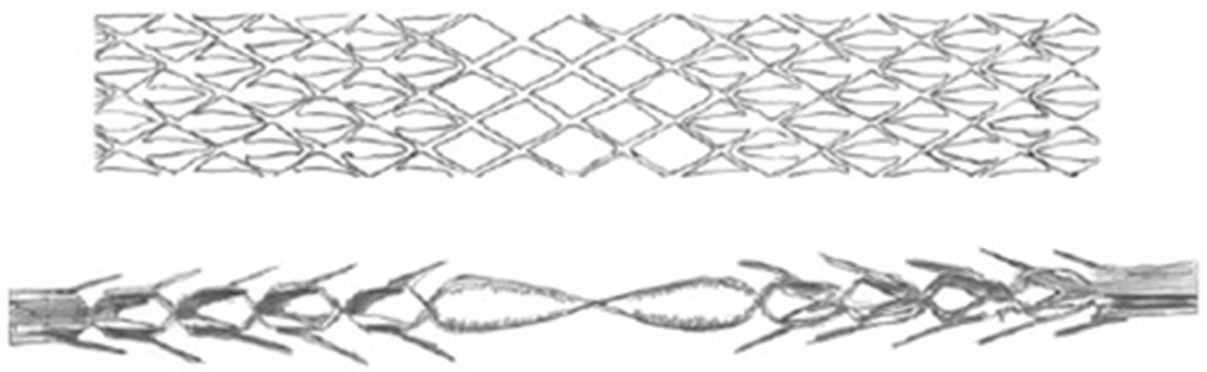
Figure 21. Nitinol tube with anchors
Finally, a device, similar to McKenzie’s and Shaw’s sutures described earlier, was introduced by QuillTM as a monofilament suture made from polypropylene, nylon and glycolic acid derivatives. It had two needles at each end with each side of the barbs being oriented away from the needle. It was primarily introduced into face lifting surgeries but is more commonly used now in sub-dermal skin closure. Silhouette suture has a resembling design and was developed by FeatherLIFT® being different than the QuillTM in having flexible, absorbable hollow cones instead of the barbs that allow the growth of tissue inside and around and thus improve the anchoring mechanism to lift the tissues [Figure 22].
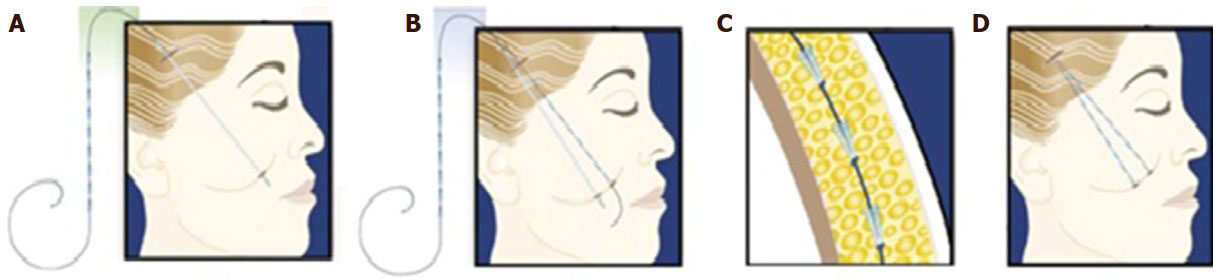
Figure 22. Face lifting procedure using the Silhouette lift threads
Considering the flexor tendons repair, in a study performed in 2005 by Lawrence and Davis[14], two factors were considered to affect the strength of the flexor tendon repair: the technique and the suture material used. Five non-absorbable 4-0 suture materials were considered: monofilament nylon (Ethicon), monofilament polypropylene (Prolene Ethicon), braided polyester (Ethibond Ethicon), braided stainless steel (Ethicon) and braided polyethylene (Fiberwire Arthrex).
A four strand flexor configuration was performed on all 150 fresh porcine flexor tendons. All repairs failed by suture rupture at the locking loop. It was observed that nylon sutures consistently produced the poorest mechanical performance in all outcome measures. Polypropylene and braided polyester showed similar results with respect to the gap formation and ultimate forces. Stainless steel and braided polyethylene sutures were significantly stronger than other suture groups. Upon exceeding the strength of the suture material, all repairs failed rather than when the holding capacity of the repair loops was exceeded. The study concluded that braided polyester is favored for core repair although some researchers prefer monofilament sutures such as nylon and polypropylene.
Another study was done by Viinikainen et al.[15] in 2004. He focused on the behavior of five flexor tendon core sutures compared by static tensile testing in vitro. The core sutures were performed with 3-0 and 4-0 braided polyester suture on fifty porcine tendons while the over running peripheral suture was done with a 6-0 monofilament polypropylene. Five different core sutures were considered as follows: Pennington modified Kessler (3-0), double Pennington modified Kessler (3-0), 4-strand Savage (3-0), 4-strand Savage (4-0) and 6-strand Savage (4-0).
The yield force and stiffness in the linear region began to increase with the number of core suture strands. It was observed that the ultimate force increased significantly when the number of strands increased or the suture caliber increased. However, the suture configuration did not influence the ultimate force. In addition, the peripheral suture contributed to the strength of the tendon repair. Thus, the tendon repair was defined as a composite of core and peripheral sutures.
Furthermore, it was observed that increasing the number of strands crossing the repair site increases the strength of the repair technique and thus averts breakage of the suture. Nevertheless, multiplying strands are also found to jeopardize the integrity of the tendon and its ability to glide. This results in adhesion formation in undesirable location and further a loss in the gliding movement of the tendon as depicted by Zhao et al.[16] in 2001.
Therefore, barbed sutures were introduced into tendon repair surgeries in an attempt to improve the strength of the repair site and without impairing the healing process. The barbs distributed along the surface of the suture are oriented in order to allow passage of the suture in one direction through the tendon tissue but exhibit resistance due to the barbs in the opposite direction. Thus, barb sutures exhibit non-slip attributes. In addition, they do not require knotting like conventional sutures; thus, failure due to knot breakage is avoided. Barb sutures are also found to reduce the straight pull tensile strength since the effective suture diameter is decreased.
In October 2009, Parikh et al.[17] performed two different suturing techniques with barb sutures, one using three and the other six strands. They compared the previous two techniques to the classical four strands suturing technique with unbarb threads. Quill 2-0 bidirectional polypropylene barb sutures were used since they demonstrated a tensile strength comparable to the 4-0 unbarb suture. This study successfully demonstrated that knotless flexor tendon repair with polypropylene barb sutures sustained equivalent or stronger forces than the unbarb, knotted repairs.
The most relevant study was the one performed by Ingle et al.[18,19], who analyzed the mechanical properties of a barb circular cross sectional suture. They concluded that rigid barbs are required for tendon repair since they can penetrate and anchor to the tissues and thus ensure a proper repair site. They reported that a cut angle of 150° with a depth of cut of 0.18 mm on a circular cross sectional suture were the most adapted parameters for the barbs when used for flexor tendon repair.
Based on all these previous experimental studies, we have performed experimentation on both circular and elliptical cross sectional sutures. Elliptical sutures were selected in order to approach the most the elliptical shape of the flexor tendon. Our experimentation and results were promising.
The two loading situations, one applied on the suture and the other on the barb itself, were considered because they represent the load to which the sutures are exposed to in vivo. Increasing the depth of cut was seen to improve the suture to sustain more loads. In addition, for the same depth of cut, the cut angle improved the behavior of sutures with elliptical cross sectional areas.
Our experimentations showed that for a depth of cut of 0.18 mm with 150° cut angle, the best elliptical cross sectional area was a/b = r = 3, while for a cut angle of 160°, the best elliptical cross sectional area was with r = 4.
These findings are crucial to invoke further research on better and improved barbed sutures with non circular cross sectional areas. The design of the barbed suture will be studied using extended finite element analysis in order to define the one which fit the best the shape of the flexor system. Also, future work can be done to account for the biological interaction of the suture with the surrounding tendon tissues. The interaction between the barb and the tendon tissues ensures a more realistic model and could provide more insights on the mode of failure. In addition more research can be performed on the best barb configuration, their arrangement and distribution over the length of the suturing wire, based on the findings done in the use of this concept in the field of aesthetic surgery[20].
Declarations
Authors’ contributionsMedical and surgical part of this work: Bakhach J, Oneissi A, Karameh R
Literature review, photos design and tables: Bakhach E
Biomechanical investigations and studies: Hantouche M, Shammas E
Data source and availabilityData in this study were derived from searches of the PubMed database.
Financial support and sponsorshipNone.
Conflicts of interestThere are no conflicts of interest.
Patient consentNot applicable.
Ethics approvalNot applicable.
Copyright© The Author(s) 2018.
REFERENCES
1. Carpenter JE, Thomopoulos S, Soslowsky LJ. Animal models of tendon and ligament injuries for tissue engineering applications. Clin Orthop Relat Res 1999;(367 Suppl):S296-311.
2. Thurman RT, Trumble TE, Hanel DP, Tencer AF, Kiser PK. Two-, four-, and six-strand zone II flexor tendon repairs: an in situ biomechanical comparisaon using a cadaver model. J Hand Surg Am 1998;23:261-5.
3. Manske PR, Gelberman RH, Vande Berg JS, Lesker PA. Intrinsic flexor-tendon repair. A morphological study in vitro. J Bone Joint Surg Am 1984;66:385-96.
5. Klein L. Early active motion flexor tendon protocol using one splint. J Hand Ther 2003;16:199-206.
6. Savage R, Risitano G. Flexor tendon repair using "six strand" method of repair and early active mobilisation. J Hand Surg Br 1989;14:396-9.
8. Jennings ER, Yeager GH. Barbwire tendon suture; clinical experience with thirty flexor tendons. AMA Arch Surg 1955;70:566-9.
9. McKenzie AR. An experimental multiple barbed suture for the long flexor tendons of the palm and fingers. Preliminary report. J Bone Joint Surg Br 1967;49:440-7.
11. Leung JC, Ruff GL, King MW, Dattilo PP. Barbed, bidirectional surgical sutures. Proceedings of International Conference & Exhibition on Healthcare and Medical Textiles; 2003 July 8-9; Bolton, United Kingdom .
12. Su BW, Protopsaltis TS, Koff MF, Chang KP, Strauch RJ, Crow SA, Rosenwasser MP. The biomechanical analysis of a tendon fixation device for flexor tendon repair. J Hand Surg Am 2005;30:237-45.
13. Hirpara KM, Sullivan PJ, O'Sullivan ME. A new barbed device for repair of flexor tendons. J Bone Joint Surg Br 2010;92:1165-70.
14. Lawrence TM, Davis TR. A biomechanical analysis of suture material and their influence on a four-strand flexor tendon repair. J Hand Surg Am 2005;30:836-41.
15. Viinikainen A, Göransson H, Huovinen K, Kellomäki M, Rokkanen P. A comparative analysis of the biomechanical behavior of five flexor tendon core sutures. J Hand Surg Br 2004;29:536-43.
16. Zhao C, Amadio PC, Momose T, Couvreur P, Zobitz ME, An KN. The effect of suture technique on adhesion formation after flexor tendon repair for partial lacerations in a canine model. J Trauma 2001;51:917-21.
17. Parikh PM, Davison SP, Higgins JP. Barbed suture tenorrhaphy: an ex vivo biomedical analysis. Plast Reconstr Surg 2009;124:1551-8.
18. Ingle NP, King MW. Optimizing the tissue anchoring performance of barbed sutures in skin and tendon tissues. J Biomech 2010;43:302-9.
19. Ingle NP, King MW, Zikry MA. Finite element analysis of barbed sutures in skin and tendon tissues. J Biomech 2010;43:879-86.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Bakhach J, Oneissi A, Bakhach E, Karameh R, Hantouche M, Shammas E. Optimization of tissue anchoring performance and mechanical properties of barbed sutures for flexor tendons repair. Plast Aesthet Res 2018;5:12. http://dx.doi.org/10.20517/2347-9264.2018.01
AMA Style
Bakhach J, Oneissi A, Bakhach E, Karameh R, Hantouche M, Shammas E. Optimization of tissue anchoring performance and mechanical properties of barbed sutures for flexor tendons repair. Plastic and Aesthetic Research. 2018; 5: 12. http://dx.doi.org/10.20517/2347-9264.2018.01
Chicago/Turabian Style
Bakhach, Joseph, Ahmad Oneissi, Elsa Bakhach, Reem Karameh, Mireille Hantouche, Elie Shammas. 2018. "Optimization of tissue anchoring performance and mechanical properties of barbed sutures for flexor tendons repair" Plastic and Aesthetic Research. 5: 12. http://dx.doi.org/10.20517/2347-9264.2018.01
ACS Style
Bakhach, J.; Oneissi A.; Bakhach E.; Karameh R.; Hantouche M.; Shammas E. Optimization of tissue anchoring performance and mechanical properties of barbed sutures for flexor tendons repair. Plast. Aesthet. Res. 2018, 5, 12. http://dx.doi.org/10.20517/2347-9264.2018.01
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 0 clicks
Cite This Article 0 clicks

 Like This Article 1
likes
Like This Article 1
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.