
Transpalpebral eyebrow lift: the mini eyebrow lift
 0
0Abstract
Aim: This paper focus is to describe and evaluate the authors' personal technique for a simplified transpalpebral eyebrow lift.
Methods: We performed surgery in 179 patients (95% females and 5% males) between years of 2008 and 2009. Initially, a thorough assessment of brow stability and symmetry was performed. To achieve desirable aesthetic we agreed upon the consensus that the eyebrow lateral third should be 0.3 to 1 cm above the supraorbital rim in women and just above or at supraorbital rim in men. Hence the surgery consisted of the removal of excess skin, treatment for bags if they were present and a transpalpebral lateral eyebrow lift.
Results: There were only 5 cases in which patients reported episodes of pain on the temporal undermined area related with the suture with the evidence of pain subsiding over time and disappearing all together within 3 months. No patients required revision surgery and no patients presented laghophtalmos or any eyelid closure difficulties.
Conclusion: This paper presents a simplified version of an eyebrow lift technique that is easy to reproduce and effective.
Keywords
Introduction
Indubitably, the upper blepharoplasty is the introductory procedure that allows surgeons from the most diverse specialties to adventure on facial cosmetic surgery. It is a procedure known to be uncomplicated, effective, quick and with high success rate. The nature of the procedure therefore sets high expectations with less understanding of the need for any potential revision surgery.
Residual fat on the medial compartment and remaining excess skin on the lateral third of the upper eyelid are probably the most common causes of patient dissatisfaction. This excess skin most of the times is not related to a conservative removal or a technique failure. Otherwise, it is caused by an undiagnosed ptosis of the lateral eyebrow [Figure 1].

Figure 1. (A) preoperative picture: patient 67 years old, male, presenting ptosis of the lateral third of the eyebrow (identified with the white arrow), not diagnosed at the time; (B) postoperative picture: 6 months after, the remaining excess skin on the lateral third of the eyebrow (identified with the white arrow) is a common cause of complaint from various patients
Generally, eyebrows are just above the superior orbital rim in men and slightly higher in women. Many patients asking for an upper blepharoplasty complain about excessive skin on the eyelid[1]. When asked to demonstrate how they would like the final result to be, patients instinctively use their hands to raise the lateral third of the eyebrow as a sign of a youthful desired result. This clearly illustrates that the problem cannot be merely a redundancy of the eyelid skin.
In this paper, the authors discuss the eyebrow position and this experience with a simple technique to be associated with the upper blepharoplasty. The authors have performed a clinical audit of 179 patients who underwent this procedure between the years of 2008 and 2009. The detailed content of the paper will also allow other surgeons to reproduce every step of the technique.
Methods
Preoperative identification of patients presenting ptosis of the lateral eyebrow is very important. In this retrospective analysis, it was confirmed that the evaluation of the position of the eyebrows was present in all preoperative consultation forms. Patients with lacrimal gland prolapse were not included in the study and can be considered a contraindication for this procedure until the prolapse is investigated and corrected. The patients were 95% female (n = 170) and 5% male (n = 9), with ages ranged between 43 and 63 years old. All patients had their surgical procedure performed with the same surgical team. They had upper blepharoplasty associated or not with other procedures (lower blepharoplasties and/or facelifts). This clinical audit followed the Declaration of Helsinki guidelines and a written consent for the outlined procedure was obtained from all patients.
An assessment of brow stability and symmetry was performed and noted in all files. Achieving a good aesthetic result begins with a careful preoperative assessment of the patient’s anatomy and desires. Nevertheless, the eyebrow lateral third should be 0.5 to 1 cm above the supraorbital rim in women[2-4]. In men, a good eyebrow position is just above or at the supraorbital rim. While performing this technique the authors aimed to achieve these reference landmarks and different fixation levels were used when asymmetric eyebrows position was diagnosed.
The surgery performed on the upper eyelid was a conventional blepharoplasty with removal of excess skin, treatment for the bags when they were present and a transpalpebral lateral eyebrow lift. During the intraoperative design of the excess skin to be resected, the surgeons marked what they would normally remove and then reduced the amount of skin to be excised on the lateral third in 2 to 4 mm, depending on the extension of lift proposed. This maneuver is paramount in order to avoid distortions on the scars positions and ultimately laghophtalmos of the lateral third of the eye. The projection of the lateral canthus is also identified as a landmark to the position of our future suture. Following marking the excess of skin to be removed, an infiltration of 20 mL lidocaine 2% associated epinephrine 1:200,000 and hyaluronidase 1500 units is performed (Hyalase, CP Pharmaceuticals, UK). The average volume of local anesthesia used is 7-10 mL for both sides and it was injected on the subcutaneous plan. Initially, only a skin flap is removed with subsequent Hemostasis, followed by a small removal of the orbicularis oculi muscle, mainly on its lateral portion. The resection of a small strip of the orbicularis muscle on its lateral portion was always performed, as it was considered to be easier to expose the orbital septum this way [Figure 2]. The surgery proceeded with the removal of the excess of fat bags when present and finally the browplasty was performed.
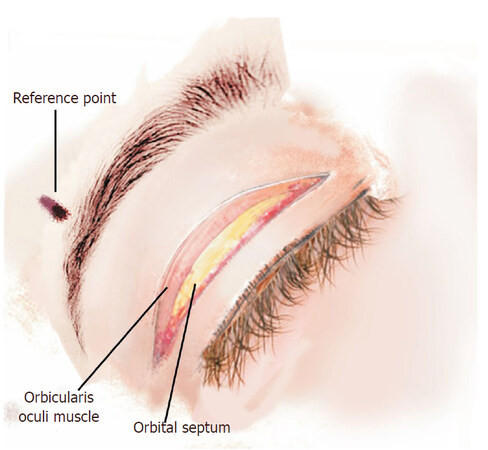
Figure 2. Artistic image of the upper eyelid after the excision of the skin and the small strip of orbicularis muscle
With the assistance of two skin hooks lifting the upper flap (with the orbicularis muscle included), it is rather easy to see the orbital rim. On the projection of the lateral corner, the surgeon initiated the dissection using a Colorado needle (Utah Medical Products, USA). The dissection is extended in the submuscular plane [Figure 3]. The dissection of a 1.5-cm semicircle cannot be too anterior, otherwise it will invade the retro-orbicularis fat (ROOF) area that is extreme vascularized and could result in excessive bleeding. On the other hand, the dissection plane cannot be too posterior as the connective tissue should be left to be used as an anchoring base for the fixation suture [Figure 4].
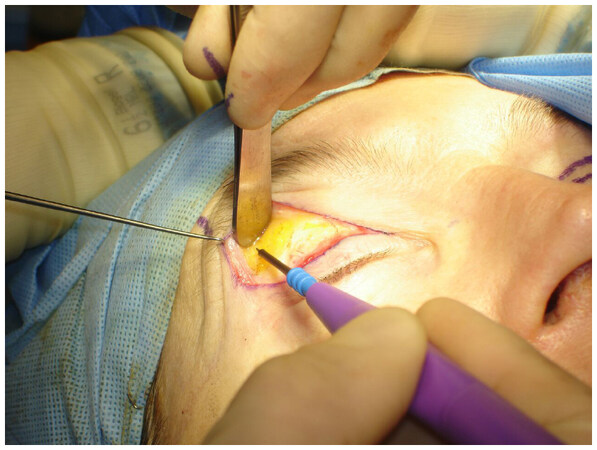
Figure 3. Picture of the initial dissection of the retro orbicularis space
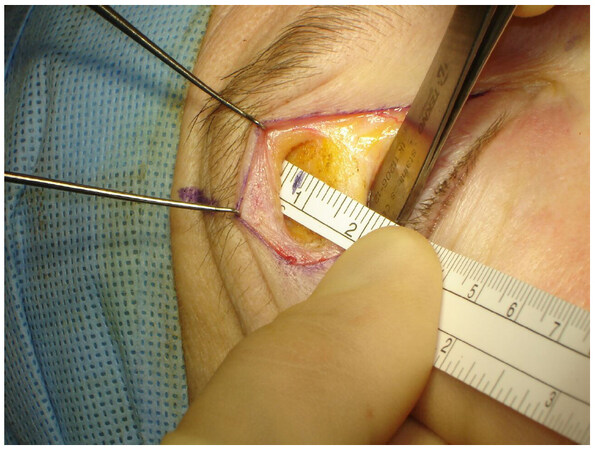
Figure 4. Picture of the retro-orbicularis space where we can measure with a simple ruler, the amount of tissue to be dissected
A Prolene 5.0 suture is inserted grabbing the periosteum with the curve of the needle parallel to the orbital rim [Figure 5]. The distance from the orbital rim is approximately 10 to 15 mm, depending on the degree of elevation desired. The degree of elevation was previously decided according to the patient’s original desire of elevation (more or less). The surgeon uses the assistance of a forceps to find the second entrance point, by pulling the skin on the junction of the projection of the lateral canthus and the lower portion of the eyebrow’s hairline. On that protrude area the suture grabs just halfway through the orbicularis muscle [Figure 6]. At this moment, prior to completing the knot, the surgeon also must verify if the suture was not too superficial and created dimples on the skin. If there were no signs of dents on the skin, the knot was completed [Figure 7]. The effect could be immediately noticed with the creation of some creases on top of the eyebrow, which will fade in 2-4 weeks [Figure 8]. The skin was closed with Nylon 6.0 continuous suture [Video 1].
[Video 1]. Edited video of the mini-eyebrow lift procedure
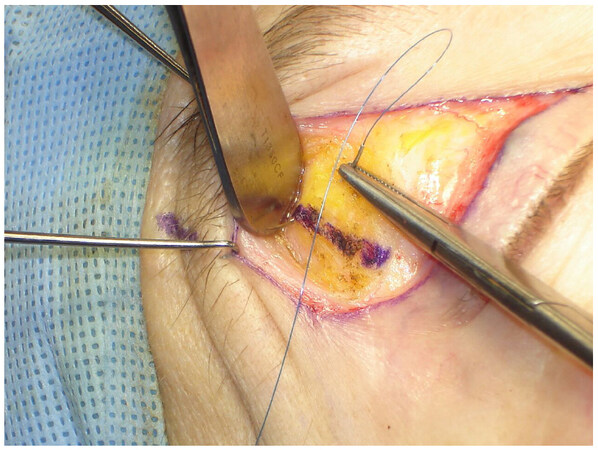
Figure 5. Picture showing the insertion of a needle capturing all the supraperiostal tissue
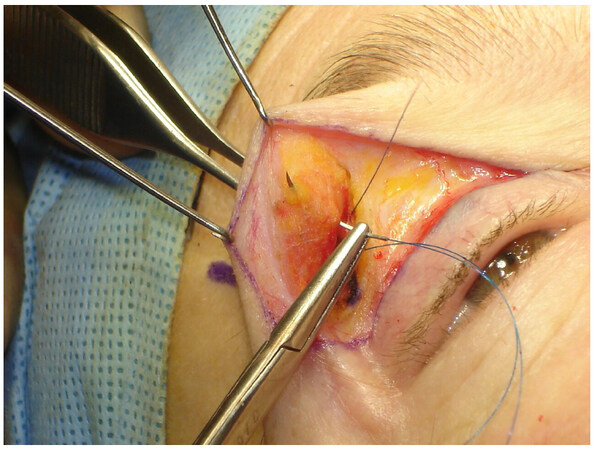
Figure 6. Picture showing the needle including only half of the thickness of the orbicularis muscle avoiding dimples on the skin
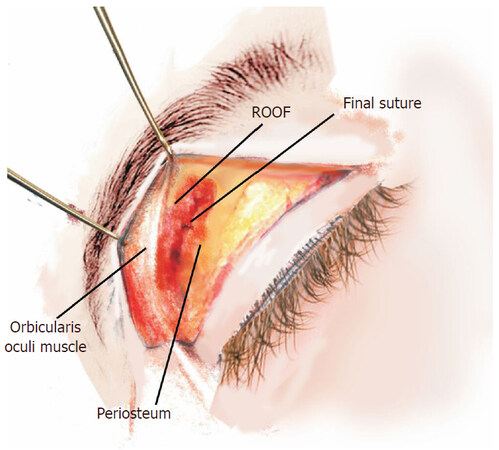
Figure 7. Artistic image of the final aspect of the suture. All the anatomical structures remain easily identifiable. ROOF: retro-orbicularis fat

Figure 8. Picture of the final aspect of the suture with the eyelid returned to its anatomical position. The evidence of lift is clear and identified with a black arrow on the picture
Results
Reviewing the present clinical audit revealed only five cases in which persistent pain was reported on the temporal undermined area related perhaps with the suture, however with the disappearing of the symptom in 2 to 3 months. No patients needed any potential revision surgery for this procedure. No patients presented laghophtalmos or any eyelid closure difficulties. Hence, a favorable result could also be confirmed with the absence of revisions as no patients returned with the complaints that the eyebrow has dropped to the original position [Figures 9 and 10]. The patients were followed up for a period of 3 months to 2 years. Additional information about patient demographics, types of procedures and complications can be found in Table 1.
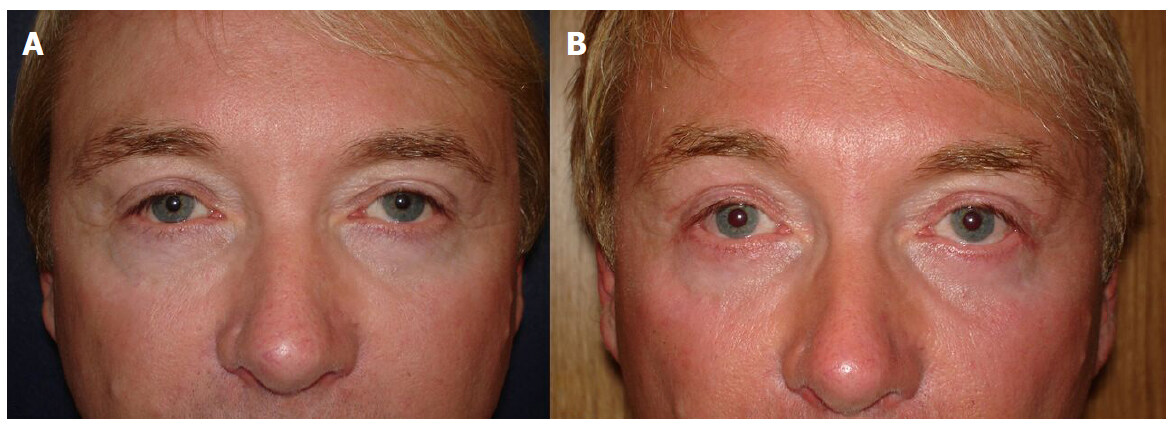
Figure 9. (A) preoperative picture: patient 52 years old, male, presenting ptosis of the lateral third of the eyebrow; (B) postoperative picture: 3 months after upper blepharoplasty with mini eyebrow lift, where we can see the satisfactory effect that the lift gives to the overall rejuvenation of the eyelid
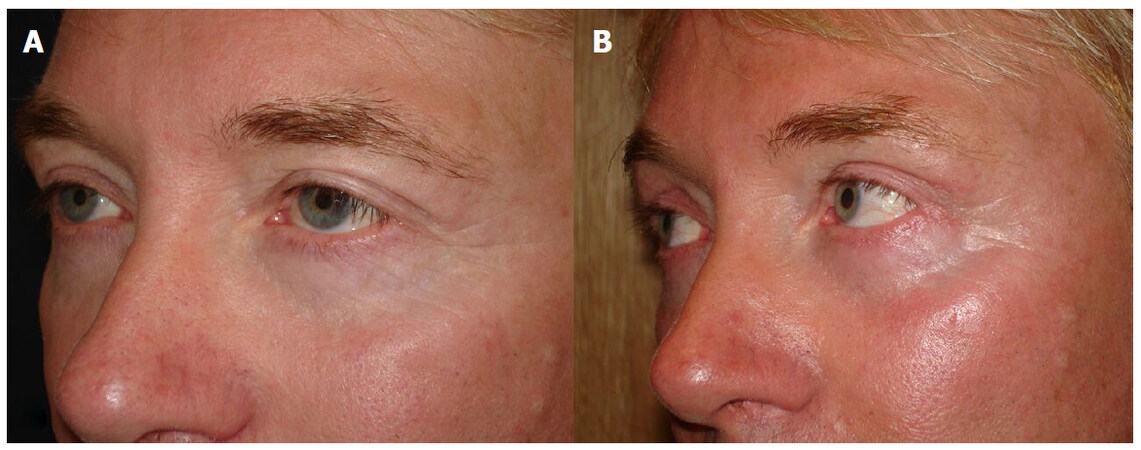
Figure 10. (A) preoperative picture: same patient with an oblique view; (B) postoperative picture: 3 months after, we can confirm the effective outcome of the mini eyebrow lift
Demographic and complications information for all patients
| Characteristics | Data |
|---|---|
| Number of patients | 179 |
| Age range (years) | 28-63 |
| Age average with SD (years) | 42.2 ± 8.28 |
| Gender | Female: 170 (95%), male: 9 (5%) |
| Postoperationpain (transient) | 5 (2.79%) |
| Seroma | 0 (%) |
| Hematoma | 0 (0%) |
| Infections | 0 (0%) |
| Wound dehiscence | 0 (0%) |
Discussion
Blepharoplasty is one of the top 5 cosmetic procedures performed in the United States with over 209,000 cases in the year of 2016[5]. Notwithstanding it’s considered a very simple procedure, there are two very common unfavorable results: remaining lateral excess of skin and medial fat bags. In the majority of upper blepharoplasties cases, the remaining excess of lateral skin is not provenient of a limited skin removal, but from an undiagnosed ptosis of the lateral portion of the eyebrow.
The desired characteristics of the eyebrows are influenced by several factors including age, gender, culture, ethnic origin and even fashion trends. However, the eyebrow’s change of position with ageing is common to all these groups. The stretching of the scalp and the laxity of the connective tissue of the frontal region is known produce a ptosis on the lateral segment before than the medial.
The first technique for eyebrow lift could possibly be attributed to Passot in 1919. Subsequently, many techniques using the coronal approach were used to correct the eyebrow ptosis. Nevertheless, it was Castañares[6] in 1964 who introduced an isolate eyebrow lift technique with world repercussion. In 1975, Hinderer[7] using a similar procedure presented the importance of the correction of the position of the eyebrow together with the upper blepharoplasty. Unfortunately, all Castañares’ like techniques lead to noticeable scars and have limited use in plastic surgeons’ practices lately.
Since 1996, Knize[8] is probably one of the few surgeons who dedicated great amount of research to the ideal eyebrow position. He also developed the first isolate eyebrow lift technique with scars hidden in the scalp, which made this procedure tremendously popular on the 90’s amongst all plastic surgeons.
Many other surgeons also emphasized the importance of the eyebrow position and several studies can be cited on the subject[9,10]. The reference measurements that were used in this technique are the result of an informal consensus found in these papers[11].
Knize’s surgery still has its important stance on the arsenal of techniques to enhance eyebrow lift. However, on the beginning of the millennium, the advances with endoscopic forehead lift could not only address the eyebrow ptosis but also could promote a full fronto-temporal rejuvenation. The complexity of endoscopic lifts still limits this procedure to a select group of surgeons and the strong market presence of toxin botulinic and fillers in hemarket immensely reduced the request for a surgical approach to the forehead. However, these non-surgical procedures are not very effective on the eyebrow ptosis.
Sokol and Sokol[12] in 1982 was the first to propose a transpalpebral browlift, eliminating forehead scars. They used a complicate interposition of flaps (muscle and periosteum) that inevitably made this technique to fall in oblivion.
In the future, papers comparing the ROOF resection with the eyebrow lift are necessary to expand the benefits of both techniques.
Albeit, McCord and Doxanas[13] in 1990 presented his transpalpebral eyebrow lift, called browplasty. His procedure consisted of a wider dissection the sub-brow space and a muscle plication with two to three mattress sutures to fixate the brow at the desired position. This very successful procedure is easily adjuncted to the conventional upper blepharoplasty and doesn’t add any extra scars to the patient. Nowadays, McCord’s procedure is probably one of the most used worldwide. In his series, it is related a prolonged brow anesthesia and paresthesia up to 6 months and also some incidence of hematoma. The authors believe that through reducing the undermined area, they could limit these complications, as no causes of permanent anesthesia or hematoma was detected.
Thereupon, many techniques have been described to promote eyebrow lift; the presented procedure is as easy to reproduce as effective. In recent years, techniques have evolved not only to improve aesthetic results but also to minimize complications. Hence, 20 years later after McCord’s original work, this paper presents a simplified version of his technique.
Declarations
Authors’ contributionsConcept and design: Sforza M
Data collection and analysis: Sforza M, Zaccheddu R
Write up: Sforza M, Sforza D
Review and final approval: Sforza M, Zaccheddu R, Sforza D
Data source and availabilityData was collected by the both senior authors’ personal series.
Financial support and sponsorshipNone.
Conflicts of interestThis work was presented by the first author as a Lecture at the ISAPS Course (International Society of Aesthetic Plastic Surgery), Almathy, 2011.
Patient consentA written consent for the outlined procedure was obtained from all patients.
Ethics approvalThis clinical audit followed the Declaration of Helsinki guidelines.
Copyright© The Author(s) 2018.
REFERENCES
2. Lazarus D. Changes in eyebrow position and shape with aging and brow lifting. Plast Reconstr Surg 2010;125:1291-2.
3. Graham DW, Heller J, Kirkjian TJ, Schaub TS, Rohrich RJ. Brow lift in facial rejuvenation: a systematic literature review of open versus endoscopic techniques. Plast Reconstr Surg 2011;128:e335-41.
5. American Society of Plastic Surgeons. National Clearinghouse of Plastic Surgery Statistics: 2008. Available from: http://www.plasticsurgery.org/documents/News/Statistics/2016/plastic-surgery-statistics-full-report-2016.pdf. [Last accessed on 15 Jan 2018].
6. Casta-ares S. Forehead wrinkles, glabellar frown and ptosis of the eyebrows. Plast Reconstr Surg 1964;34:406-13.
8. Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg 1996;97:1321-33.
9. Langsdon PR, Williams GB, Rajan R, Metzinger SE. Transblepharoplasty brow suspension with a biodegradable fixation device. Aesthet Surg J 2010;30:802-9.
10. Georgescu D, Anderson RL, McCann JD. Brow ptosis correction: a comparison of five techniques. Facial Plast Surg 2010;26:186-92.
11. Codner MA, Kikkawa DO, Korn BS, Pacella SJ. Blepharoplasty and brow lift. Plast Reconstr Surg 2010;126:e1-17.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Sforza M, Zaccheddu R, Sforza D. Transpalpebral eyebrow lift: the mini eyebrow lift. Plast Aesthet Res 2018;5:2. http://dx.doi.org/10.20517/2347-9264.2017.35
AMA Style
Sforza M, Zaccheddu R, Sforza D. Transpalpebral eyebrow lift: the mini eyebrow lift. Plastic and Aesthetic Research. 2018; 5: 2. http://dx.doi.org/10.20517/2347-9264.2017.35
Chicago/Turabian Style
Sforza, Marcos, Renato Zaccheddu, Deborah Sforza. 2018. "Transpalpebral eyebrow lift: the mini eyebrow lift" Plastic and Aesthetic Research. 5: 2. http://dx.doi.org/10.20517/2347-9264.2017.35
ACS Style
Sforza, M.; Zaccheddu R.; Sforza D. Transpalpebral eyebrow lift: the mini eyebrow lift. Plast. Aesthet. Res. 2018, 5, 2. http://dx.doi.org/10.20517/2347-9264.2017.35
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 7 clicks
Cite This Article 7 clicks

 Like This Article 38
likes
Like This Article 38
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.