
A mammometric comparison of modified Robertson versus Wise pattern inferior pedicle reduction mammoplasty

Abstract
Aim: The advent of 3D photoimaging and mammometrics has allowed for quantitative, volumetric breast analyses. This study uses 3D photoimaging and mammometrics to compare the postoperative morphometric outcomes of the modified Robertson technique to the more traditional Wise pattern inferior pedicle technique.
Methods: Inferior pedicle reduction mammoplasty was performed using either a Wise pattern or modified Robertson skin incision. 3D photography and analysis were done at 1-3 months and 6-12 months postoperatively.
Results: There were 14 breasts in the modified Robertson group (ROB) and 24 breasts in the Wise pattern group (WISE). There were no significant differences in demographic data or amount of tissue resected. At 6-12 months, the modified Robertson cohort demonstrated increased superior pole fullness (62.9% ROB vs. 58.3% WISE, P = 0.05). The Wise cohort, however, maintained greater maximum breast projection (5.52 cm ROB vs. 6.54 cm WISE, P = 0.01) and increased medial pole fullness (29.6% ROB vs. 46.9% WISE, P < 0.01). There was no difference in tissue shifting from the superior pole to the inferior pole over time (+3.36 superior pole % ROB vs. +1.42 superior pole % WISE, P = 0.28). Areola surface area increased equally in both cohorts (+3.08 cm2 ROB vs. +2.59 cm2 WISE, P = 0.77); however, the final size of the areola was greater in the modified Robertson cohort (26.9 cm2 ROB vs. 21.6 cm2 WISE, P < 0.01).
Conclusion: Using 3D mammometrics, we found increased superior pole fullness in the modified Robertson group while the Wise pattern group demonstrated greater medial pole fullness and maximum breast projection.
Keywords
Introduction
Reduction mammoplasty is one of the most commonly performed operations in plastic surgery and has some of the highest patient reported levels of satisfaction.[1-5] The inferior pedicle Wise pattern technique is considered the “gold standard” due to its consistently reproducible results, even in large reductions;[2,6,7] however, critics of the technique describe the final result as wide, flat, “boxy” in appearance, and lacking in superior pole fullness.[8] More importantly, over time, this technique has been shown to undergo tissue redistribution from the superior to inferior pole. This phenomenon is referred to as pseudoptosis and further exacerbates the lack of superior pole fullness.[2,9-11]
The Robertson technique was first described in 1964[12-14] as an alternative to free nipple grafting in massive reductions. Later modifications incorporated a bell-shaped incision followed by the development of a superior apron flap to lower the position of the transverse bell-shaped scar.[15] These modifications eliminated the vertical midline scar found in the Wise pattern, while offering greater flexibility to manipulate and shape the breast inferior pedicle. Proponents also claim that the modified Robertson technique allows for greater nipple projection, improved preservation of the inframammary crease, and less pseudoptosis.[3,16]
While the use of linear measurements can be used as a proxy for pseudoptosis and changes over time, the advent of 3D photography and stereophotogrammetry has allowed for volumetric measurement and objective analysis of breast outcomes.[17-19] The use of 3D mammometrics has been validated over the last decade, and has been established in the analysis of breast reductions.[20-23]
This study uses 3D breast photography and mammometrics to compare postoperative volumetric and morphologic outcomes between modified Robertson and Wise pattern inferior pedicle breast reductions. Specifically, we aim to compare postoperative superior pole fullness, pseudoptosis, and breast projection over time. Other measurements with clinical and aesthetic relevance include sternal notch to nipple distance, nipple to inframammary fold (IMF) distance, inter-nipple distance, areola surface area, total breast volume, and medial pole fullness. This is the first quantitative analysis comparing these two different skin resection patterns for the inferior pedicle breast reduction.
Methods
After obtaining Institutional Review Board approval, patients seeking breast reduction operations between 2012 and 2014 were invited to participate in this study. Patients were randomly assigned by the scheduling department to either surgeon A, who used a modified Robertson skin incision pattern, or surgeon B, who used a Wise pattern. Exclusion criteria included age less than 18 years or more than 65 years, the history of breast surgery, the history or presence of breast malignancy, and the significant weight change affecting breast volume during the course of the study. Outlier patients with extreme body mass index (BMI) (> 40 kg/m2 or < 26 kg/m2), postoperative breast volume at early postoperative time point (< 400 mL or > 1,300 mL), and the weight of breast tissue resected (< 400 g or > 1,300 g) were also excluded.
Both surgeons marked patients in the standing position preoperatively, placing the nipple position at Pitanguy’s point. In the modified Robertson cohort, the IMF incision was then determined 8 cm below the new nipple position and marked accordingly. Intraoperatively, the new IMF marking was used to elevate a superior breast apron down to the chest wall. The inferior pedicle was created with a base width of 12-16 cm, depending on the length of the nipple to IMF. Once the pedicle was defined, the intervening tissue was removed, and the apron was draped over the pedicle with transposition of the nipple. In the Wise cohort, the pedicle width was 10-12 cm, and the vertical skin incision was made 6-7 cm below the areola.
After the surgery, 3D photographs (Canfield Vectra 3D Camera) were taken during the early postoperative period (1-3 months postoperatively) and the late postoperative period (6-12 months postoperatively). Patients who did not return for both photographs were removed from the study. Complications were recorded during these follow-up visits, including painful scars, wound dehiscence, infection requiring antibiotics, and surgical revision.
Mammometric and volumetric breast analyses were completed using Geomagic software. Important landmarks were consistently marked on all images. These included sternal notch, nipple, and point of maximum breast projection. The point of maximum projection was defined as the point maximally projected on the Z-axis on a lateral, profile view of the breast. The nipple was usually also the point of maximum projection but this did not hold true in all cases. Linear measurements recorded include sternal notch to nipple surface distance, internipple vector distance, nipple to IMF surface distance, and projection of the breast from the chest wall to the nipple and point of maximum breast projection.
Surface area measurements recorded include the areola. Volumetric measurements recorded include total breast volume, percent volume in superior pole, and percent volume in medial pole. The borders of the breast were defined using the anterior axillary line as the lateral boundary, the sternal midline as the medial boundary, the IMF as the inferior boundary, and the chest wall as the dorsal boundary. Percent superior pole volume was defined as volume of the breast superior to an YZ axial plane through the point of maximum projection divided by total breast volume. Percent medial pole volume was defined as volume of the breast medial to a XZ sagittal plane through the point of maximum projection divided by total breast volume.
Statistical analysis was completed using Statistical Package for the Social Sciences. Independent samples t-tests and chi-squared tests (Fischer’s exact) were used where appropriate and a P ≤ 0.05 was considered statistically significant. With an estimated 3% effect size in the modified Robertson group and 6% in the inferior pedicle group for tissue movement to the inferior pole, a common standard deviation of 2, a 0.5 level of significance, and a 0.8 power level, the sample size was calculated to be 7 in each cohort.
Results
Twenty-two patients consented and completed the required components of the study. Two patients were excluded as outliers due to excessive BMI and excessive volumes resected, and 1 patient was excluded due to low BMI. In total, there were 14 measured breasts in the modified Robertson cohort (ROB) and 24 breasts in the Wise cohort (WISE).
No statistically significant differences were found between the 2 cohorts regarding age (36.9 years ROB vs. 38.5 years WISE, P = 0.74), BMI (33.9 kg/m2 ROB vs. 30.9 kg/m2 WISE, P = 0.08), total breast volume (809 mL ROB vs. 729 mL WISE, P = 0.26), or the weight of breast tissue resected (695 g ROB vs. 712 g WISE, P = 0.84; Table 1). Complications requiring surgical revision were minimal (Fisher’s exact test: 2/14 ROB vs. 0/24 WISE, P = 0.13). The 2 complications were both dog-ears that developed at the late postoperative period and revised under local anesthesia. Preoperative 3D photographs were not taken or analyzed due to the limitations of the software to accurately measure massive breasts with ptosis resting on the abdominal wall.
Demographic statistics
| ROB (range) | WISE (range) | P value | |
|---|---|---|---|
| Age (years) | 36.9 (30-41) | 38.5 (21-65) | 0.74 |
| BMI (kg/m2) | 33.9 (31.1-37.2) | 30.9 (26.4-35.7) | 0.08 |
| Total breast volume (mL) | 809 (459-1,080) | 729 (555-1,253) | 0.26 |
| Tissue resected (mL) | 695 (406-1,000) | 712 (449-1,280) | 0.84 |
Early postoperative period
In the early postoperative period [Table 2], sternal notch to nipple distance was not significantly different between the 2 cohorts (23.1 cm ROB vs. 23.7 cm WISE, P = 0.24); however, nipple to IMF was significantly greater in the modified Robertson cohort (12.3 cm ROB vs. 10.6 cm WISE, P < 0.01). Internipple distance was not significantly different between the 2 cohorts (23.6 cm ROB vs. 21.6 cm WISE, P = 0.17). Nipple projection was not significantly different between the 2 cohorts (5.91 cm ROB vs. 6.97 cm WISE, P = 0.10); however, maximum breast projection was greater in the Wise cohort (5.55 cm ROB vs. 6.69 cm WISE, P = 0.01). Areola surface area was greater in the modified Robertson cohort (23.6 cm2 ROB vs. 19.0 cm2 WISE, P < 0.01).
Early postoperative period
| ROB (range) | WISE (range) | P value | |
|---|---|---|---|
| SNtoNIP (cm) | 23.1 (20.1-25.3) | 23.7 (20.9-25.6) | 0.24 |
| NIPtoIMF (cm) | 12.3 (9.3-15.3) | 10.6 (8.4-12.9) | 0.00* |
| NIPtoNIP (cm) | 23.6 (15.5-27.7) | 21.6 (17.0-24.6) | 0.17 |
| NipProj (cm) | 5.91 (2.15-8.70) | 6.97 (5.09-9.26) | 0.10 |
| MaxProj (cm) | 5.55 (4.09-8.64) | 6.69 (4.67-9.26) | 0.01* |
| AreolaSA (cm2) | 23.8 (21.3-28.1) | 19.0 (13.17-24.05) | 0.00* |
| BreastSA (cm2) | 490 (388-571) | 422 (355-547) | 0.00* |
| TotVol (mL) | 809 (459-1,081) | 729 (555-1,253) | 0.26 |
| SupPole% | 59.6 (45.7-69.4) | 56.9 (44.2-66.6) | 0.21 |
| MedPole% | 27.0 (20.5-50.2) | 45.5 (31.2-63.1) | 0.00* |
Total breast volume was not significantly different between the two cohorts (809 mL ROB vs. 729 mL WISE, P = 0.26). Percent volume in the superior pole was not different between the 2 cohorts (59.6% ROB vs. 56.9% WISE, P = 0.21); however, percent volume in the medial pole was greater in the WISE cohort (27.0% ROB vs. 45.5% WISE, P < 0.01).
Late postoperative period
In the late postoperative period [Table 3, Figure 1], sternal notch to nipple distance was not significantly different between the 2 cohorts (24.4 cm ROB vs. 24.1 cm WISE, P = 0.57); however, nipple to IMF remained significantly greater in the modified Robertson cohort (13.2 cm ROB vs. 10.8 cm WISE, P < 0.01). Interestingly, internipple distance became significantly different during the late postoperative period (24.8 cm ROB vs. 21.3 cm WISE, P < 0.01). Nipple projection was not significantly different between the 2 cohorts (6.59 cm ROB vs. 6.70 cm WISE, P = 0.83); however, maximum breast projection remained greater in the Wise cohort (5.52 cm ROB vs. 6.54 cm WISE, P = 0.01). Areola surface area remained greater in the modified Robertson cohort (26.9 cm2 ROB vs. 21.6 cm2 WISE, P < 0.01).
Late postoperative period
| ROB (range) | WISE (range) | P value | |
|---|---|---|---|
| SNtoNIP (cm) | 24.4 (21.4-26.4) | 24.1 (21.5-26.4) | 0.57 |
| NIPtoIMF (cm) | 13.2 (10.3-15.9) | 10.8 (8.3-14.2) | 0.00* |
| NIPtoNIP (cm) | 24.8 (22.5-27.6) | 21.3 (17.3-23.6) | 0.00* |
| NipProj (cm) | 6.59 (3.18-9.00) | 6.70 (4.65-9.18) | 0.83 |
| MaxProj (cm) | 5.52 (4.08-7.46) | 6.54 (4.50-8.77) | 0.01* |
| AreolaSA (cm2) | 26.9 (16.3-37.1) | 21.6 (12.9-33.7) | 0.02* |
| BreastSA (cm2) | 494 (402-593) | 419 (344-559) | 0.00* |
| TotVol (mL) | 856 (486-1,183) | 709 (489-1,123) | 0.06 |
| SupPole% | 62.9 (51.1-73.6) | 58.3 (42.3-69.9) | 0.05* |
| MedPole% | 29.6 (20.3-42.1) | 46.9 (34.2-62.9) | 0.00* |
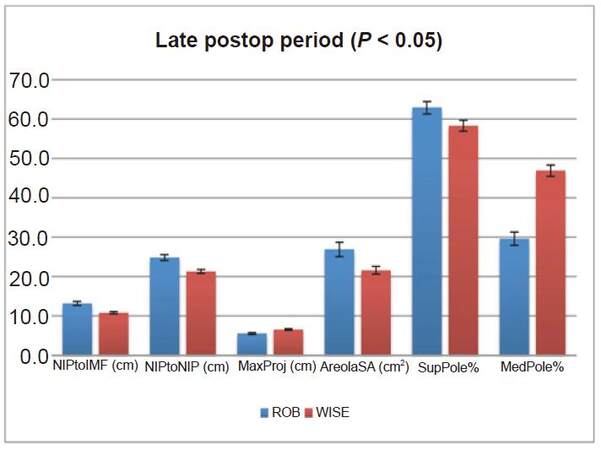
Figure 1. Late postoperative period significant findings (all P < 0.05). Statistically significant differences during the late postoperative period between the modified Robertson and Wise pattern cohorts. Y-axis displays units in cm, cm2, and %, depending on the variable. X-axis displays the name of the variable presented with the units in parenthesis. ROB cohort is represented by blue bars and WISE cohort is represented by red bars. Error bars show standard error. Nipple to inframammary fold distance (NIPtoIMF) was greater in the ROB cohort than the WISE cohort. Internipple distance (NIPtoNIP) was greater in the ROB cohort than the WISE cohort. Maximum breast projection (MaxProj) was greater in the WISE cohort than the ROB cohort. Areola surface area (AreolaSA) was greater in the ROB cohort than the WISE cohort. % volume in the superior pole (SupPole%) was greater in the ROB cohort than the WISE cohort. % volume in the medial pole (MedPole%) was greater in the WISE cohort than the ROB cohort
Total breast volume was not significantly different between the 2 cohorts (856 mL ROB vs. 709 mL WISE, P = 0.06). Interestingly, the percent volume in the superior pole was greater in the Robertson cohort (62.9% ROB vs. 58.3% WISE, P = 0.05), while percent volume in the medial pole remained greater in the WISE cohort (29.6% ROB vs. 46.9% WISE, P < 0.01).
Comparing changes over time between modified Robertson vs. Wise cohorts
Analyzing the change over time (late postoperative measurement minus early postoperative measurement) between the two cohorts [Table 4, Figures 2 and 3], modified Robertson cohort patients experienced greater lengthening of both the sternal notch to nipple distance (1.31 cm ROB vs. 0.44 cm WISE, P < 0.01) and the nipple to IMF distance (0.88 cm ROB vs. 0.27 cm WISE, P = 0.05). While internipple distance increased 1.20 cm in the modified Robertson cohort and decreased 0.26 cm in the Wise cohort, this difference did not reach statistical significance (P = 0.09). Nipple projection increased significantly more in the modified Robertson cohort than the Wise cohort (0.69 cm ROB vs. -0.26 cm WISE, P < 0.01); however, there was no difference in the change in maximum breast projection between the two cohorts (-0.02 cm ROB vs. -0.15 cm WISE, P = 0.67). Areola size increased in both the modified Robertson and Wise cohorts, but this increase was not significantly different between the two cohorts (3.08 cm2 ROB vs. 2.59 cm2 WISE, P = 0.77).
Change over time
| ROB (range) | WISE (range) | P value | |||
|---|---|---|---|---|---|
| SNtoNIP (cm) | 1.31 (0.60-2.31) | 0.44 (-0.52-2.10) | 0.00* | ||
| NIPtoIMF (cm) | 0.88 (-1.25-3.26) | 0.27 (-0.76-1.82) | 0.05* | ||
| NIPtoNIP (cm) | 1.20 (-1.21-6.98) | -0.26 (-1.66-0.87) | 0.09 | ||
| NipProj (cm) | 0.69 (-0.80-2.00) | -0.26 (-2.15-1.81) | 0.00* | ||
| MaxProj (cm) | -0.02 (-1.85-1.43) | -0.15 (-2.24-2.01) | 0.67 | ||
| AreolaSA (cm2) | 3.08 (-7.13-9.81) | 2.59 (-3.86-10.14) | 0.77 | ||
| BreastSA (cm2) | 4.00 (-31.83-50.46) | -2.89 (-29.50-36.55) | 0.28 | ||
| TotVol (mL) | 46.7 (-112.7-170.5) | -20.1 (-168.1-216.5) | 0.04* | ||
| SupPole% | 3.36 (-4.06-7.82) | 1.42 (-11.16-22.05) | 0.28 | ||
| MedPole% | 2.57 (-8.16-12.39) | 1.36 (-17.94-17.96) | 0.60 | ||
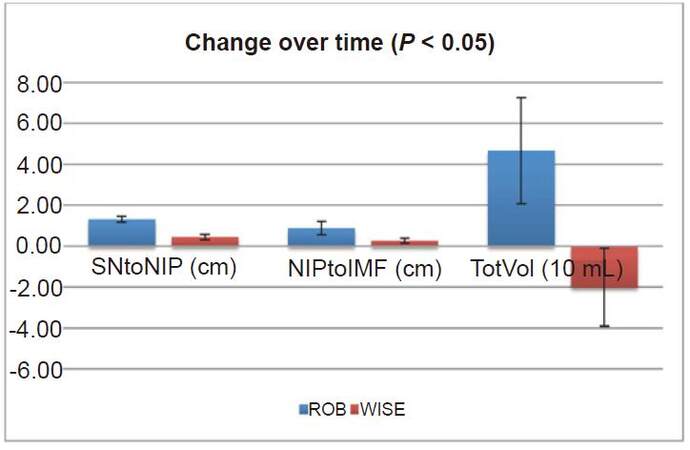
Figure 2. Change over time significant findings (all P < 0.05). Statistically significant differences from the early postoperative period to the late postoperative period between the modified Robertson and Wise pattern cohorts. Y-axis displays units in cm and 10 mL, depending on the variable. X-axis displays the name of the variable presented with the units in parenthesis. ROB cohort is represented by blue bars and WISE cohort is represented by red bars. Error bars show standard error. The change in sternal notch to nipple distance (SNtoNIP) was greater in the ROB cohort than the WISE cohort. The change in nipple to inframammary fold distance (NIPtoIMF) was greater in the ROB cohort than the WISE cohort. The change in total volume (TotVol) increased in the ROB cohort but decreased in the WISE cohort
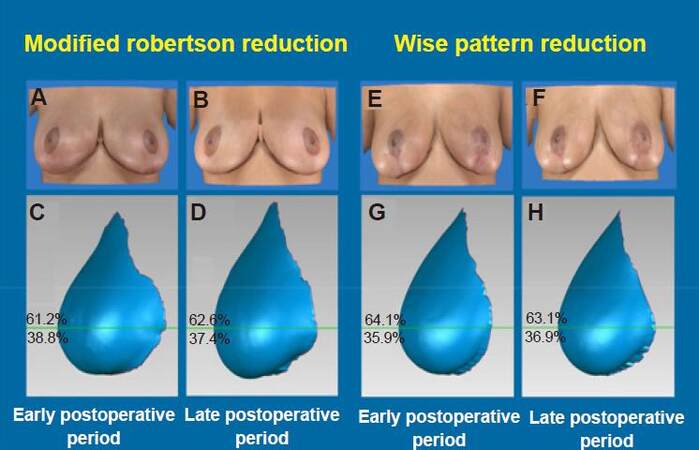
Figure 3. Example images. Patient photographs and 3D reconstruction images showing volumetric analysis. Images A-D are from the same ROB patient (age: 31 years) and images E-H are from the same WISE patient (age: 26 years). (A) AP photograph of ROB breasts at early postoperative time period; (B) AP photograph of ROB breasts at late postoperative time period; (C) 3D reconstruction lateral view of left breast of ROB patient at early postoperative period showing 61.2% superior pole volume; (D) 3D reconstruction lateral view of left breast of ROB patient at late postoperative period showing superior pole volume of 62.6%; (E) AP photograph of WISE breasts at early postoperative time period; (F) AP photograph of WISE breasts at late postoperative time period; (G) 3D reconstruction lateral view of left breast of WISE patient at early postoperative period showing 64.1% superior pole volume; (H) 3D reconstruction lateral view of left breast of WISE patient at late postoperative period with superior pole volume of 63.1%
Interestingly, total volume increased in the modified Robertson cohort but decreased in the Wise cohort; this difference was statistically significant (46.7 mL ROB vs. -20.1 mL WISE, P = 0.04). The change in percent superior pole volume was greater in the modified Robertson cohort (3.36%) than the Wise cohort (1.42%); however, this difference did not reach statistical significance (P = 0.28). The change in percent medial pole volume (2.57% ROB vs. 1.36% WISE, P = 0.60) was not significantly different between the two cohorts.
Discussion
This study is the first to use 3D mammometrics to provide quantitative analysis comparing the modified Robertson and Wise patterns for inferior pedicle reduction mammoplasty. Movassaghi et al.[15] directly compared the two skin patterns in breast reduction; however, their analysis focused on complication rates of hematoma, minor wound dehiscence, and scar hypertrophy. They found a reduced complication rate in the modified Robertson technique with decreased skin breakdown, since this skin pattern does not have an intersecting triple point. Chalekson et al.[3] evaluated morphologic outcomes of modified Robertson patients; however, they compared the results to aesthetically optimal breasts, instead of other reduction patients. Their recorded outcomes included patient satisfaction, symptom reduction, scarring, nipple position, ptosis, pseudoptosis, shape, and overall appearance several years following surgery. They found excellent satisfaction among patients and no difference between their reduction patients and aesthetically ideal patients with regards to pseudoptosis.
Using 3D analysis to compare the late postoperative result of the modified Robertson to the Wise pattern breast reduction, the modified Robertson technique demonstrated greater superior pole volume by approximately 5%. This difference was both statistically and clinically significant. Previous research by Mallucci et al.[24] analyzed breast photographs with 5% differences in superior to inferior pole ratio to determine ideal breast shape, finding that the 45:55 ratio was aesthetically preferred over the 50:50 ratio. It is possible that the superior breast apron of the modified Robertson technique supports the inferior pedicle and maintains superior pole volume without the presence of a vertical incision in the Wise pattern technique.
In addition, the Wise technique demonstrated greater medial pole volume by approximately 17% and greater maximum breast projection by 1 cm. The presence of a vertical scar may distribute the inferior pedicle medially and narrow the width of the breast, leading to improved breast projection. The vertical incision may also prevent lateral migration of the nipple position as demonstrated by the smaller internipple distance in the Wise pattern cohort (21.3 cm WISE vs. 24.8 cm ROB, P < 0.01).
The total breast volume of the modified Robertson cohort increased over time (+47 mL), whereas the Wise cohort decreased (-20 mL). It is possible that these changes reflect systemic changes in the patient with weight and/or menstrual cycle. This change in total volume is consistent with an increase in notch to nipple and nipple to IMF measurements in the modified Robertson cohort. An increase in overall volume of the breast may also explain the increase in nipple projection found in the modified Robertson cohort. In contrast, the Wise cohort had a decrease in total volume over time, which is also consistent with the decrease in nipple projection and maximum breast projection.
The modified Robertson cohort consistently demonstrated longer nipple to IMF distances compared to the Wise pattern, and this can be explained by the surgeon preference to widen the skin bridge of the breast apron below the areola to minimize ischemic complications.
The areola surface area was consistently larger in the modified Robertson cohort compared to the Wise pattern cohort at all time points. Both surgeons reported using the same 38 mm “cookie cutter” when insetting the areola; however, the superior breast apron of the modified Robertson places greater tension and outward pull on the areola compared to the Wise pattern. Despite these absolute differences, the areola surface area in both cohorts increased equally over time. The inferior pedicle may apply pressure and weight behind the areola that results in similar expansion over time.
Although statistically significant, some of the measured differences between the two cohorts were clinically small and may seem within the margin of error for 3D analysis. This error in 3D analysis is the result of limitations of 3D photography and minor computational inaccuracies in the software. This is especially true when measuring the lower pole and determining the IMF in patients with extremely ptotic breasts. However, we firmly believe that these measurements are valid since each image was measured three times, averaged, and pooled with other images within the same cohort. User dependent differences in making measurements can also lead to inaccuracies in 3D analysis; however, all measurements were performed by the same person, who had extensive experience performing 3D analysis. This study is also adequately powered as determined by the sample size calculation and the fact that the results were statistically significant.
This report represents the outcomes of individual surgeons at one institution and considering that there are many technical variations within each technique, the results may not be generalizable to all surgeons. It is possible that the variation in surgical technique, rather than the chosen skin incision pattern, has a greater impact on volumetric distribution. Further study of other surgeons who perform these techniques could determine reproducibility of our results. Future studies could also evaluate whether further morphologic changes occur in the 6-12 month time frame. Larger sample sizes will also help to further support our findings.
In conclusion, using 3D mammometrics, our results suggest that in the late postoperative period, the modified Robertson technique provides increased superior pole fullness, whereas the Wise technique provides increased medial pole fullness and maximum breast projection. These quantitative results allow plastic surgeons to choose the technique that may be most suitable for a patient seeking reduction mammoplasty.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
Patient consent
Obtained.
Ethics approval
Approved by the Institutional Review Board.
REFERENCES
1. American Society of Plastic Surgeons. 2013 Plastic Surgery Statistics Report. Available from: http://www.plasticsurgery.org/Documents/news-resources/statistics/2013-statistics/plastic-surgery-statistics-full-report-2013.pdf [Last Accessed on 23 July 2015].
2. Spear SL. Surgery of the breast principles and art. Philadelphia, United States: Lippincott Williams & Wilkins; 2006.
3. Chalekson CP, Neumeister MW, Zook EG, Russell RC. Outcome analysis of reduction mammaplasty using the modified Robertson technique. Plast Reconstr Surg 2002;110:71-81.
4. Collins ED, Kerrigan CL, Kim M, Lowery JC, Striplin DT, Cunningham B, Wilkins EG. The effectiveness of surgical and nonsurgical interventions in relieving the symptoms of macromastia. Plast Reconstr Surg 2002;109:1556-66.
5. Strong B, Hall-Findlay EJ. How does volume of resection relate to symptom relief for reduction mammaplasty patients? Ann Plast Surg 2015;75:376-82.
6. Wise RJ. A preliminary report on a method of planning the mammaplasty. Plast Reconstr Surg 1956;17:367-75.
7. Courtiss EH, Goldwyn RM. Reduction mammaplasty by the inferior pedicle technique. An alternative to free nipple and areola grafting for severe macromastia or extreme ptosis. Plast Reconstr Surg 1977;59:500-7.
8. Hall-Findlay EJ. Vertical reduction mammaplasty. In: Thorne CH, editor. Grabb and Smith's Plastic Surgery. 7th Ed. Philadelphia, USA: Lippincott Williams & Wilkins; 2014.
9. Hudson DA, Geldenhuys S, Duminy F, Adams K. Another look at breast projection after breast reduction. Aesthetic Plast Surg 2008;32:928-32.
10. Shiffman MA. Mastopexy and breast reduction principles and practice. Berlin, Germany: Springer; 2009.
11. Hall-Findlay EJ. Pedicles in vertical breast reduction and mastopexy. Clin Plast Surg 2002;29:379-91.
12. Robertson DC. Reduction mammaplasty using a large inferior flap. Transactions of Third International Congress of Plastic Surgery. Washington DC, United States: Excerpta Medical Foundation; 1964.
14. Robertson DC. Follow-up clinic: the technique of inferior flap mamma-plasty. Plast Reconstr Surg 1973;52:438.
15. Movassaghi K, Liao EC, Ting V, Matros E, Morris DJ, Orgill DP, Pribaz JJ. Eliminating the vertical scar in breast reduction-Boston modification of the Robertson technique. Aesthet Surg J 2006;26:687-96.
16. Zook EG, Sommer NZ. The Modified Robertson Reduction Mammaplasty. Mastopexy and Breast Reduction: Principles and Practice. Berlin, Germany: Springer; 2009. pp. 483-7.
17. Kovacs L, Eder M, Hollweck R, Zimmermann A, Settles M, Schneider A, Udosic K, Schwenzer-Zimmerer K, Papadopulos NA, Biemer E. New aspects of breast volume measurement using 3-dimensional surface imaging. Ann Plast Surg 2006;57:602-10.
18. Kovacs L, Eder M, Hollweck R, Zimmermann A, Settles M, Schneider A, Endlich M, Mueller A, Schwenzer-Zimmerer K, Papadopulos NA, Biemer E. Comparison between breast volume measurement using 3D surface imaging and classical techniques. Breast 2007;16:137-45.
19. Losken A, Seify H, Denson DD, Paredes AA, Carlson GW. Validating three-dimensional imaging of the breast. Ann Plast Surg 2005;54:471-8.
20. Quan M, Fadl A, Small K, Tepper O, Kumar N, Choi M, Karp N. Defining pseudoptosis (bottoming out) 3 years after short-scar medial pedicle breast reduction. Aesthetic Plast Surg 2011;35:357-64.
21. Small KH, Tepper OM, Unger JG, Kumar N, Feldman DL, Choi M, Karp NS. Re-defining pseudoptosis from a 3D perspective after short scar-medial pedicle reduction mammaplasty. J Plast Reconstr Aesthet Surg 2010;63:346-53.
22. Tepper OM, Unger JG, Small KH, Feldman D, Kumar N, Choi M, Karp NS. Mammometrics: the standardization of aesthetic and reconstructive breast surgery. Plast Reconstr Surg 2010;125:393-400.
23. Tepper OM, Small K, Rudolph L, Choi M, Karp N. Virtual 3-dimensional modeling as a valuable adjunct to aesthetic and reconstructive breast surgery. Am J Surg 2006;192:548-51.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Zhu VZ, Shah A, Lentz R, Sturrock T, Au AF, Kwei SL. A mammometric comparison of modified Robertson versus Wise pattern inferior pedicle reduction mammoplasty. Plast Aesthet Res 2016;3:284-90. http://dx.doi.org/10.20517/2347-9264.2016.48
AMA Style
Zhu VZ, Shah A, Lentz R, Sturrock T, Au AF, Kwei SL. A mammometric comparison of modified Robertson versus Wise pattern inferior pedicle reduction mammoplasty. Plastic and Aesthetic Research. 2016; 3: 284-90. http://dx.doi.org/10.20517/2347-9264.2016.48
Chicago/Turabian Style
Zhu, Victor Z., Ajul Shah, Rachel Lentz, Tracy Sturrock, Alexander F. Au, Stephanie L. Kwei. 2016. "A mammometric comparison of modified Robertson versus Wise pattern inferior pedicle reduction mammoplasty" Plastic and Aesthetic Research. 3: 284-90. http://dx.doi.org/10.20517/2347-9264.2016.48
ACS Style
Zhu, VZ.; Shah A.; Lentz R.; Sturrock T.; Au AF.; Kwei SL. A mammometric comparison of modified Robertson versus Wise pattern inferior pedicle reduction mammoplasty. Plast. Aesthet. Res. 2016, 3, 284-90. http://dx.doi.org/10.20517/2347-9264.2016.48
About This Article
Copyright

Data & Comments
Data


 Cite This Article 0 clicks
Cite This Article 0 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.